What Causes Elbow Pain?
M3 India Newsdesk Jul 29, 2022
Elbow pain is commonly caused by a relatively small number of conditions that include periarticular (tendinitis and bursitis), articular (arthritis), bone (fracture and dislocation), or neurologic problems. The history, causes and treatment of elbow pain are elucidated in this article.
Key takeaways
- Approaching elbow pain.
- Causes of elbow pain.
- Bedside tests which are helpful in the diagnosis of elbow pain.
- Exercises that can help prevent worsening of elbow pain.
- Medical management of elbow pain.
Elbow pain evaluation
Evaluation of elbow pain focuses on answering three important questions:
- Is there evidence of major trauma or injury?
- Can symptoms and signs be adequately explained by a local problem confined to the elbow?
- Is there evidence of a more generalised articular process, of which the elbow is only a part of a neurologic process with elbow symptoms referred from another site?
The elbow joint is formed by the articulation of the distal end of the humerus with the proximal radius and ulna. The normal arc of motion ranges from full extension (0 degrees) to full flexion (135 degrees). Some individuals demonstrate the ability to extend the elbow beyond normal; this condition is referred to as "cubitus recurves" or cubital recurvatum.
Multiple bursae have been identified around the elbow joint; the olecranon bursa is the most superficial, and swelling of this bursa is both common and easily observed.
Noting patient history
History is very important in identifying the cause of the pain. The type of pain, whether it is radiating or localised is very important. The onset of the injury and a history of prior interventions, for example, surgeries, rehabilitative therapy and injections may offer important insights into aetiology. A mnemonic used for characterising pain in almost any site is OPQRST: O = onset, P = precipitating (and ameliorating) factors, Q = quality, R = radiation, S = severity, and T = timing
Initial assessment:
The two most basic steps in examining joints are inspection and palpation:
- Inspection- It includes noting skin changes (erythema, rash, swelling) from the front and behind both. Also to look for any deformity in the form of cubits varus or valgus (seen in deforming arthritis like RA) and also to look for nodules in the elbow like seen in rheumatoid arthritis and gout.
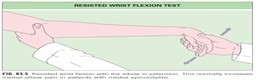
- Palpation- It includes the range of motions of the joint ( flexion/extension) and (supination/pronation) and palpating both the epicondyles to look for medical and lateral epicondylitis. Special tests to look for medial and lateral epicondylitis are resistance wrist extension and resisted wrist flexion tests as shown below.

Causes of elbow pain
| Lateral elbow (extensor) tendinopathy |
| Loose bodies |
| Osteochondral defect (radiocapitellar joint) |
| Arthritis (posterior osteophytes) |
| Valgus extension overload |
| Radial tunnel syndrome |
| Inflammatory arthritis |
| Lateral synovial plica |
| Cervical radiculopathy |
| Thoracic outlet syndrome |
| Myofascial pain |
Differential diagnosis for lateral elbow pain
| Medial elbow (flexor) tendinopathy |
| Cubital tunnel syndrome |
| Ulnar neuritis |
| UCL insufficiency |
| Little league elbow |
| Inflammatory arthritis |
| Cervical radiculopathy |
| Thoracic outlet syndrome |
| Myofascial pain |
| UCL: ulnar collateral ligament |
Differential diagnosis for medial elbow pain
Common disorders of the elbow
1. Olecranon bursitis
One of the rare bursae where palpable swelling and irritation and inflammation manifest as clinically obvious is the olecranon bursa. The two most common inflammatory conditions affecting the olecranon bursa are rheumatoid arthritis and gout.
The most clinically urgent problem involving the bursa is septic olecranon bursitis which is commonly confused with septic arthritis. patients with septic arthritis will usually have severe pain with limited elbow flexion and extension.
Range of motion is surprisingly preserved in patients with septic cellulitic olecranon bursitis. Gentle, passive elbow extension is perhaps the most useful discriminating manoeuvre to help differentiate between these two possibilities
2. Lateral epicondylitis
Patients with lateral epicondylitis, also called tennis elbow, usually complain of localised pain and tenderness at the lateral epicondyle, often accompanied by a mild aching discomfort in the proximal forearm.
Patients with lateral epicondylitis usually have an insidious onset of pain over weeks to months. On careful questioning, most will associate lifting heavy objects (milk cartons, hammers, suitcases) with increased pain.
On occasion, actions as simple as shaking hands will provoke symptoms. Localized tenderness is present just distal, medial, and slightly anterior to the lateral epicondyle, over the common extensor tendon, particularly that part derived from the extensor carpi radialis brevis muscle.
3. Medial epicondylitis
Medial epicondylitis, or the so-called golfer’s elbow, is far less common than lateral epicondylitis. Insertional tendinitis at the medial epicondyle may result from swimming, baseball pitching, or golfing. It is often associated with aching discomfort in the medial epicondyle and flexor aspect of the proximal forearm. It is increased by lifting, grasping, and other activities that require frequent wrist flexion and forearm pronation. There is tenderness at and just distal to the medial epicondyle over the origin of the common flexor tendon.
Treatment plans
The treatments described can be categorized as those for short-term pain relief, for example, pain medications, forearm brace, local injections and those for improving the long-term health of the tendons, for example, eccentric strength exercises.
1. Exercises
There are stretch exercises which can be done for improving the Tennis elbow and Golfer’s elbow showed in image 1 and image 2 respectively. These exercises can be done twice a day and most important is holding the particular position for 30 seconds.
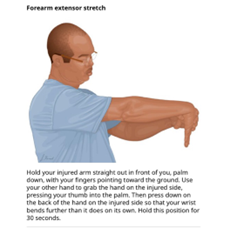
Image 1

Image 2
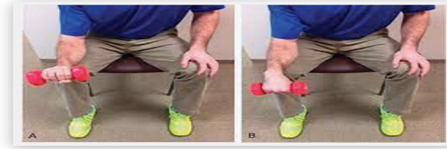
2. Eccentric strength exercises
These exercises have been effectively used in the management of tendinopathies in multiple regions of the body. The patient has to use the free hand to bend the affected wrist back as far as the patient can while lifting the weight and lower the hand with it as seen in the picture. These exercises help slow muscle contractions and strengthen muscles.
3. Medications
Most of these conditions improve with:
- Conservative management
- Wait & watch (80 % improve spontaneously)
- Symptomatic treatment- Can be given in the form of NSAIDs and intralesional steroid therapies
Physical therapies in the form of mulligan’s mobilisation done by physiotherapists may be helpful. Surgical management can be considered the last option in which the Nirschl procedure, Arthroscopic tennis elbow surgery can be done. Other therapies helpful are USG therapy, Acupuncture etc.
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author is a DNB resident in rheumatology from Manipal hospital.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
