What every GP should know about the best pain relief technique
M3 India Newsdesk Feb 07, 2022
Clinicians often come across scenarios where they have to make decisions on using anaesthetic blocks. Discussed here is a case-based scenario that poses a question of which would be the best method of pain management when a patient walks in with an injury.
A case at a GP clinic
A 40-year-old gentleman is brought into the clinic in obvious agony. He sustained a major injury to his right foot, including all three toes, while doing agricultural chores. Nursing receives normal vital signs, with the exception of some minor tachycardia. Access to an IV is gained. After confirming that the patient has no allergies, 6-mg of morphine is immediately delivered.
Head to toe evaluation and analysis of systems finds no additional injuries apart from the right first through third toe amputations, with all three amputations happening through the proximal phalanxes with protruding bone fragments and well-controlled bleeding. The patient makes no reference to previous medical history.
You immediately determine that this is an open fracture and place an IV prescription for cefazolin and gentamicin. When a re-evaluation indicates that the patient is still in extreme agony, you repeat the morphine. As the orthopaedic surgeon is now occupied with another case in the OR, it will likely be another 2-3 hours before he can see the patient.
Meanwhile, the patient's nurse approaches and informs you that the patient's pain has not been much reduced by the repeated morphine. You repeat the morphine, but wonder what your following steps in pain management should be.
Regional blocks
In the simplest terms, regional blocks are achieved by injecting lidocaine or bupivacaine near a peripheral nerve. Therefore, when do you do it? Indications include the following:
- Injuries where local infiltration is not possible
- Injuries where excessive local anaesthetic is required
- Injuries where local infiltration impedes closure or impairs blood flow
- Injuries where local infiltration would result in increased pain (foot/hand)
Anaesthetic agent for regional blocks- It is necessary to identify the proper anaesthetic for regional blocks.
- Bupivacaine (0.25 per cent) has a longer duration of action (2-9 hours)
- Lidocaine (1%), which has a shorter duration of action (10-40 minutes)
Theoretically, there is a danger of vasospasm related to adrenaline mixed with local anaesthetic in end arteriole circumstances such as the fingers, nose, or penis.
General considerations for regional blocks (irrespective of type)
- Aseptically prepare the field.
- Take sterile measures if working near a joint, vessel, or contaminated region.
- Infiltrate with a 25- or 27-gauge needle.
- Always aspirate while advancing the needle.
- Know where your code cart is in case of lidocaine toxicity.
Landmarks:
- Direct yourself using tendons, bones, and other landmarks of paresthesia. This is subjective and needs patient cooperation (once provoked, withdraw the needle 1 to 2 mm before injecting).
- Nerve stimulator connects to needle and induces spasms in linked muscles when in close proximity to the nerve.
- In the realm of nerve blocks, ultrasound is your best buddy.
- Ultrasound enables you to monitor your needle at all times and the anaesthetic's distribution.
Ankle block
An ankle block would be the most appropriate in this instance. Essentially, the foot is innervated by five nerves. You may restrict the nerves you wish to block depending on the location of the foot that is hurt if you know your anatomy.
Equipment- You'll need the following for the basic blocks:
- Your preferred anaesthetic
- Syringe (5-10 ml)
- Blunt fill needle
- 23-27 gauge needle
- Antiseptic wipe
| Blocks | Parts covered | Technique |
| Posterior tibial nerve block | The sole of the foot | Palpate the posterior tibial artery behind the medial malleolus. Inject 3-5 ml of anaesthetic 1-cm in-depth 1-cm superior to this point. |
| Block | 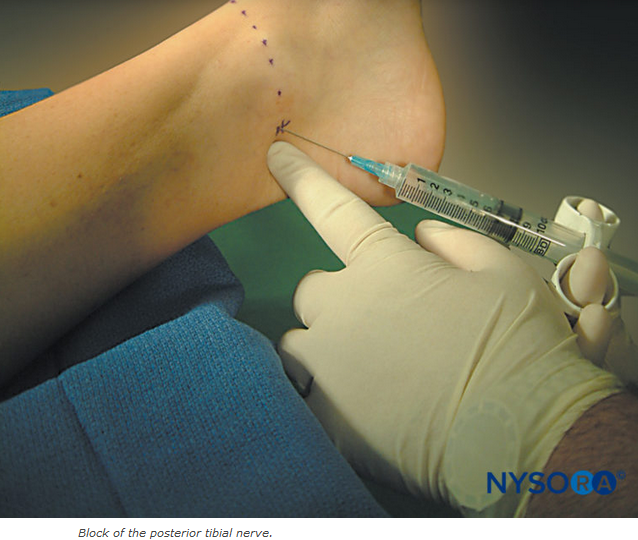 |
|
| Sural nerve block | Posterior and lateral foot |
Inject 3-5-mL of anaesthetic subcutaneously in a band between the Achilles tendon and 1-cm above the lateral malleolus.
|
| Superficial peroneal nerve block | Dorsal aspect of the foot and toes |
Inject 4-10-ml of anaesthetic subcutaneously in a band between the lateral malleolus and the extensor hallucis longus tendon.
|
| Deep peroneal nerve block | Just the area between the big toe and the second toe |
Have the patient dorsiflex their foot and insert the needle 1-cm above the medial malleolus aiming underneath the extensor hallucis longus tendon and advance until you hit the tibia. Then inject 3-5-ml of anaesthetic.
|
| Saphenous nerve block | Medial aspect of the foot |
Inject 2-5-ml subcutaneously between the medial malleolus and the anterior tibial tendon.
|




- In terms of risk-benefit analysis, whenever we discuss lidocaine (or other local/regional anaesthetics), we should also include systemic toxicity associated with local anaesthetics.
- Common complications are peri-oral numbness, metallic taste, paraesthesia, tinnitus, and disorientation. Serious complications include coma, seizure, or cardiac toxicity.
- Toxicity variables include the drug (bupivacaine is the most toxic), the dosage, the pace of administration, the injection location, and the presence or absence of a vasoconstrictor.
Doses- The following totals are not to be exceeded (with reference to optimal body weights):
- Bupivacaine (0.25 per cent) without adrenaline: 2 mg/kg
- Bupivacaine (0.25 per cent) in combination with adrenaline: 3 mg/kg
- Lidocaine (1%) without adrenaline: 4 mg/kg
- Lidocaine (1%), combined with adrenaline: 7 mg/kg
Management
Supportive care and benzodiazepines for seizures, ACLS algorithms for cardiac issues, however, lipoinfusion is required in the end.
Revisiting the case
Despite having taken 16 milligrammes of morphine in the last 50 minutes, the patient's discomfort persists. You ponder switching opioids or initiating a PCA while continuing to manage the patient's pain, but instead, choose to do an ankle block fast. The patient quickly reports feeling better. He is finally transferred to the operating room, where his incision is cleaned and skin flaps are performed.
Pain relief is the thing that gives immense satisfaction to the patient when he visits the doctor.
“Simple regional block is the best tonic for suffering.”
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author is a practising super specialist from New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
