Vesico Ureteric Junction [VUJ] Obstruction in Children
M3 India Newsdesk Jul 16, 2024
This article describes the causes, diagnosis, and treatments for Vesico Ureteric Junction (VUJ) obstruction, which can lead to hydroureteronephrosis, megaureter, and renal damage.
UTI in children
Urinary tract infections are common in youngsters. Although there are relatively few symptoms and indicators that are particular to urinary tract infections, infants and female children are more likely to get UTIs.
Urinary tract infections are more common in young girls and infants. However, youngsters are also predisposed to UTIs by a number of other underlying risk factors. These could include urological conditions like the following that have a mechanical obstruction in the urinary tract:
- Pelvic-ureteric junction [PUJ] obstruction
- Vesicoureteric junction [VUJ] obstruction
- Posterior urethral valves [PUV]
VUJ obstruction
Obstruction at the level of Vesico Ureteric Junction [VUJ] can lead to hydroureteronephrosis [dilated ipsilateral renal pelvis and ureter] and megaureter [abnormally dilated ureter] and subsequent renal damage.
The causes for obstruction at the level of VUJ include:
- Intrinsic abnormality of the distal ureter
- Ureterocele either of a single or complex duplex system
- Megaureters with both VUR and kinking distal ureteric obstruction
- Intraluminal stones obstructing VUJ
1. The intrinsic abnormality of the distal ureter
- This is rare and true stenosis is rarely reported. During cystoscopy, the ureteric orifice appears normal in such cases. A ureteral catheter or stent can be passed in some cases thereby relieving the obstruction.
- However, if the ureteric orifice is too narrow this may not be possible. Reimplantation of the distal ureter to another site within the bladder restores the flow of urine and the success rates are very good.
2. Ureterocele and duplex renal system
Ureterocele is a saccular dilatation of the distal intravesical ureter. It can be unilateral or bilateral and may be associated with duplex renal systems. Most of the ureteroceles are contained within the bladder and termed intravesical. However, they can also be seen extending outside the bladder and called extravesical.
Intravesical ureteroceles usually distend and obstruct the flow of urine distally from the ureter to the bladder. However, they can also lead to VUR if the ureteric orifice is widely open. How and why ureteroceles develop is still uncertain and embryological causes are implicated.
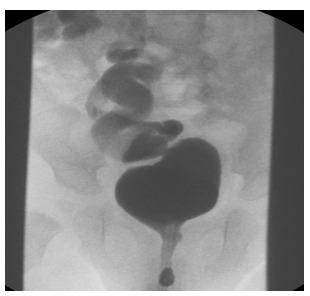
Figure 1: MCUG showing duplex system on the right side with Grade 4 VUR in the lower moiety ureter. Reflux is also demonstrated in the distended right upper moiety ureter.
In children, ureteroceles are more common in girls than boys. The left side is slightly more common than the right side. Almost 10% of the ureteroceles are bilateral. Although ureteroceles can occur in isolation, most of the ureteroceles seen in children are associated with the duplex renal system. In the duplex system, there are two ureters draining two poles of the kidney independently.
The lower pole ureter is normally placed and usually associated with VUR, while the upper pole ureter is ectopic and most commonly associated with ureteroceles. The upper moiety ureters are usually obstructed with the ureterocele, however, in some cases can be associated with VUR as well [Figure 1].
The majority of these upper pole kidneys are associated with renal dysplasia implying that abnormal induction of blastema has taken place leading to defective nephrogenesis.
Antenatal ultrasound scans can detect hydroureteronephrosis and raise the suspicion of ureteroceles. Postnatal Ultrasound Imaging can detect ureteroceles and is a useful screening tool. A ureterocele appears as a well-defined cystic intravesical mass extending to the distal ureter. Intravenous urogram can also detect ureteroceles.
But this requires a functioning renal unit and therefore in the duplex system the ureteroceles are not seen as the associated upper renal moiety is usually non-functional. The same problem exists with nuclear imaging studies like DMSA and MAG3 scans.
Direct examination during cystoscopy can reveal more than one ureteric orifice on one side and thereby suggest a duplex renal system. MCUG can also reveal ureterocele and is commonly used [Figure 2].
Asymptomatic neonates diagnosed antenatally in the absence of severe hydroureteronephrosis are at low risk of developing urinary tract infections and therefore antibiotic prophylaxis and regular monitoring might suffix..
In patients with severe hydroureteronephrosis, the upper pole renal function dictates the need for surgical correction of ureteroceles. If the upper pole renal function is salvageable an open surgical approach or endoscopic decompression of the ureterocele is done. Hydroureteronephrosis in patients with associated VUR the correction is more complex.
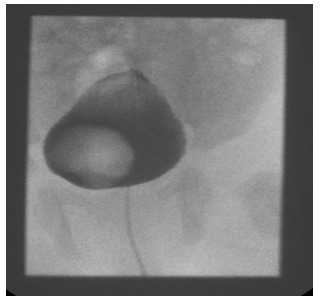
Figure 2: MCUG showing a ureterocele seen as a filling defect on the right side of the urinary bladder. No associated VUR is seen
3. Megaureters
- Abnormally dilated ureters are referred to as Megaureters. In general, there are two types of megaureters. The first type is associated with massive reflux as seen in grade 4 and 5 VUR and the second type is associated with obstruction as seen with ureterocele and ectopic ureters. It should be noted that most megaureters detected are secondary to VUR alone rather than VUJ obstruction.
- However, both VUR and VUJ obstruction can co-exist as a one-way valve-like mechanism resulting in huge megaureters. Very rarely as seen in Prune-belly syndrome the ureter musculature is at fault with excessive connective tissue and resulting in megaureter.
- In all the cases of megaureter, the resultant stasis of urine predisposes to UTI and subsequent renal damage. Correction of megaureter is addressed by correcting the underlying abnormality along with tapering the distal ureter and refashioning the VUJ.
4. Distal ureteric stones
Urinary stones [urolithialis] are relatively less common than seen in adults. Most urinary stones in children are seen in the renal pelvis and produce PUJ obstruction.
Rarely do the stones pass down the ureter and get obstructed at the level of the distal ureter. The stones can be a consequence of UTI or due to altered contents of urine excreted by the kidneys.
Metabolic disorders include:
- Hypocitraturia (42%)
- Hyperoxaluria (32.1%)
- Hypercalciuria (25%)
- Hyperuricosuria (9.8%)
- Cystinuria (2.7%)
This has been reported in 92% of the cases in children and therefore should be ruled out before surgical intervention. In children, distal ureteric stones of ≤ 3 mm diameter are likely to pass spontaneously, and stones of ≥ 4 mm are unlikely to do so and may benefit from early intervention.
The management of ureteral stones in children is becoming more similar to that in adults and extracorporeal shock wave lithotripsy (ESWL) and YAG laser lithotripsy are commonly used.
Click here to read about Pelvic-Uteric Junction [PUJ] Obstruction in Children.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Sivasankar Jayakumar is MBBS, MRCS, FEBPS, Department of Paediatric Surgery & Urology, Apollo Cradle & Children’s Hospital, Karapakkam, Chennai.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
