Treatment approach for PCOS and infertility: Dr Sonia Malik
M3 India Newsdesk Jun 17, 2020
Dr. Sonia Malik throws light on a very vital topic- PCOS and infertility and explains the Indian Fertility Society recommendations for treatment of the condition.

Polycystic Ovary Syndrome (PCOS) is an enigmatic endocrinal disorder first described by Stein Levinthal in 1932. [1] With a better understanding of the cause and the evolution of the disease, the diagnosis and the management have undergone many changes. It is now known that this condition can present variously in different patients and each type has to be treated differently.
The diagnosis of PCOS from the infertility perspective essentially pertains to recognising the phenotype so that specific and adequate treatment can be initiated.
Clinico-pathological basis of infertility
PCOS is a metabolic disorder with endocrinal ramifications leading to heterogenous presentations. It is essentially a genetic disorder, influenced by environmental and dietary factors. The genetic basis of the disorder translates into derangements in the insulin metabolism or malfunctioning of LH, or both. These abnormalities result in excessive production of androgens leading to a state of hyperandrogenemia and an accompanying anovulation. This in turn affects the ovaries that enlarge in size and volume and appear polycystic due to the trapped follicles in various stages of development. Hence, it is the degree and type of endocrinal derangement that defines the PCOS phenotype and the resultant infertility. The three described cardinal features according to the Rotterdam [2] criteria are:
- Anovulation
- Hyperandrogenimia
- Polycystic appearance of the ovaries
Two out of the three criteria if present, qualify the patient as having PCOS. Since these symptoms are present in varying combinations, the resultant phenotypes are also many and varying: [3]
- Hyperandrogenic, anovulatory, and PCOM (classical or frank PCOS): Most common of all phenotypes among patients of PCOS, this is the most severe form and consists of all the three features. It therefore requires aggressive treatment.
- Hyperandrogenic and anovulation (metabolic phenotype or non-PCO PCOS): In this phenotype, presence of androgen excess is demonstrable clinically or/and biochemically along with presence of oligomenorrhoea. The prevalence and incidence of IGT and DM2 are consistently high in this phenotype across various racial groups. The odds of having IGT are 1.6 folds and DM2 are 4 folds higher than normal controls matched for age and weight.
- Hyperandrogenic or PCOM but normal ovulation (or ovulatory PCOS): This the second most common phenotype among PCOS patients. It is associated with normal insulin sensitivity. This is a low-severity phenotype that is easy to treat and gives a good prognosis on lifestyle modification. Women of this phenotype are lean.
- Normoandrogenic anovulation and PCOM (normoandrogenic PCOS): This phenotype is only recognised by Rotterdam criteria– high probability of normal insulin sensitivity, but may have higher LH levels and low SHBG levels.
The last two phenotypes are essentially milder, and may not be easily identifiable clinically. However, they present with slightly different clinical complaints and symptoms. PCOM is common to both and aggressive ovarian stimulation can land them in OHSS.
Tests for infertility and PCOS
- Since a majority of the patients present with irregular cycles or ammenorrhoea, it essentially means testing for anovulation and categorising the patient according to the WHO classification for anovulation. Tests pertaining to this need to be carried out.
- The fundamental basis is the metabolic problem associated with obesity and high androgens, hence, tests to rule out other causes of hyperandrogenimia must be done in order to institute proper treatment.
- Hyperinsulinemia is a clinical diagnosis and hence signs like acanthosis nigrans must be looked for. No test is recommended to diagnose it. However, an oral glucose tolerance test (OGTT) or blood sugar is recommended in order to rule out diabetes and metabolic syndrome in such patients. Blood pressure must also be checked in all cases of PCOS.
- An ideal BMI is a favourable indicator in PCOS. High BMI indicates more metabolic involvement and a lean PCOS on the other hand would have a high LH and a high AMH or both with some hyperinsulinimia.
The recommended diagnostic workup in sub-fertile women with PCOS would therefore be as follows:
- Clinical determination of two of the three Rotterdam criteria (including AFC)
- AFC on U/S scan
- Biochemical determination of baseline FSH, LH, AMH
- Testosterone and 17-hydroxyprogesterone in women with hirsutism and negative progesterone withdrawal bleed
- Serum prolactin and TFT
- Blood sugar, OGTT
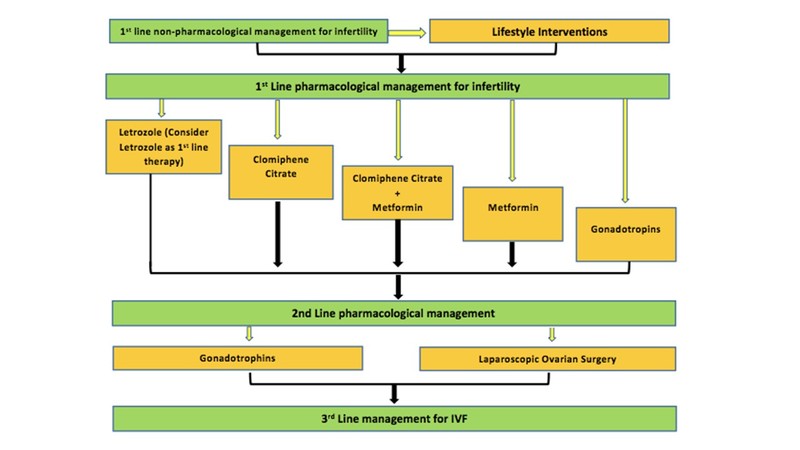
Treatment
Pretreatment counseling is fundamental when it comes to treatment of some of these women with severe form of disease. Diet and exercise form the mainstay of treatment. The Indian Fertility Society [4] outlined recommendations for the treatment of PCOS based on the Indian need. They are as follows:
Recommendations on lifestyle intervention for management of subfertility in PCOS [4]
- Lifestyle modifications targeted at weight reduction (at least 5%) or prevention of weight gain are recommended as first-line therapy before attempting pharmacological methods of OI in sub-fertile women with PCOS. (Grade A, EL 1)
- Lifestyle modification should include calorie restriction with any hypocaloric diet (reduced by 500 kcal/day) and physical activity of 60 min/day up to 3 months along with restriction of other risk factors- excessive caffeine intake, alcohol consumption, and smoking. (Grade A, EL 2)
- The duration of lifestyle management interventions can be decreased in age-related decline in fertility. (Grade B, EL 4)
- In morbidly obese (BMI >35 kg/m2) PCOS patients, pharmacological methods of OI should be avoided before weight reduction. (Grade B, EL 4)
- Yoga is recommended as a part of lifestyle management workup. (Grade B, EL 3)
- The treatment with Orlistat is recommended under medical supervision in the event of unsuccessful weight reduction with diet and exercise alone for 2 to 3 months in morbidly obese patients. (Grade B, EL 1)
Recommendations on use of bariatric surgery
- Bariatric surgery is recommended as second-line treatment in morbidly obese (BMI >30 kg/m2) PCOS patients who are unsuccessful in achieving weight reduction by lifestyle modification. (Grade B, EL 4)
- In patients with BMI >50 kg/m2, bariatric surgery is suggested as first-line therapy for weight reduction. (Grade B, EL 4)
- It is recommended to avoid conception for at least 12 months after bariatric surgery because the effects of these interventions on the evolution of early pregnancy are not yet known. (Grade B, EL4)
Recommendations on pretreatment with combined oral contraceptive pill (COCP)
- Low-dose combined COCPs pretreatment (with or without lifestyle modifications) for at least 2 months is recommended in patients with high LH level (three times the basal levels) to normalise it. (Grade B, EL 4)
Recommendations on use of aromatase inhibitors
Aromatase inhibitors are now considered as first-line dugs when pharmacological treatment is considered for OI in these patients.
- In anovulatory and sub-fertile PCOS patients with CCR with no other sub-fertility factors, administration of AIs (letrozole 2.5 mg/day for 10 days) is suggested as first line or after CC resistance or failure.
- In patients with breast cancer and PCOS requiring oocyte cryopreservation, AIs are recommended.
PCOS women administered with AIs should be counseled about the risk of congenital malformations.
Recommendations on clomiphene citrate
CC was considered as first-line for a long time but is not favoured now due to CC resistance and low pregnancy rate.
- In anovulatory PCOS, CC is recommended as a first-line pharmacological agent at a starting dose of 50 mg/day starting from day 2 of the menstrual cycle for 5 days. The maximum recommended dose of CC for OI is 150 mg/day, and increased by 50 mg/day at each cycle for a maximum of six cycles. (Grade A, EL 1)
- Ultrasound monitoring should be offered to infertile PCOS women who are on CC for monitoring ovulatory response and to minimise the risk of multiple pregnancies. In an event of unavailability of ultrasound, monitoring of LH levels can be another alternative. (Grade B, EL 3)
Recommendations on insulin sensitising agents
Metformin is recommended in the following circumstances:
- In PCOS patients with impaired glucose intolerance (disturbed oral glucose tolerance test)
- In obese PCOS women co-administered with clomiphene
- In CC-resistant PCOS women
- In PCOS women who are at high risk of hyperstimulation
It is recommended to start with a dose of 500 mg daily with the main meal of the day for 1 to 2 weeks, followed by an increase of 500 mg/day weekly or biweekly if required, until a maximum dose of 2500 to 2550 mg/day is reached. If side effects worsen with increased dose, the current dose is maintained for 2 to 4 weeks until tolerance is developed.
Recommendations on gonadotropins and GnRH analogs
- Gonadotropins are recommended as a second-line treatment for not exceeding three ovulatory cycles in PCOS women with CCR or for failure to conceive in those who are anovulatory and with no other sub-fertility factors. (Grade A, EL 2)
- When gonadotropins are indicated, it is recommended to counsel patients on the need for strict monitoring of cycle, the risk of OHSS and multiple pregnancy, the cost of treatment, and cycle cancellation criteria before treatment initiation. (Grade B, EL 4)
- When gonadotropins are indicated, the low-dose step-up protocol is recommended over step-down protocol to reduce the chances of OHSS in PCOS patients with sub-fertility. (Grade A, EL 2)
- The recommended starting dose of gonadotropin is 37.5 to 50.0 IU/day for 7 to 10 days, with small dose increments of 50% of the initial or previous dose if follicle ≥12 mm is not developed, and ovulation is triggered when there is the development of a leading follicle ≥18 mm in size. (Grade B, EL 4)
Recommendations on laparoscopic surgery
This is an optional second-line management in a select group of patients. The main indications for the use of LOD in women with anovulatory PCOS, as an alternative to gonadotropins are:
- CCR
- Persistent hypersecretion of LH, either during natural cycles or in response to CC
- The need for laparoscopic assessment of their pelvis
- Poor access to healthcare facilities (living far or other practical reasons) for intensive monitoring required during gonadotropin therapy
Recommended in-
- In anovulatory PCOS women who are CCR and have hypersecretion of LH levels with no other sub-fertility factors, as second-line therapy over gonadotropin therapy (Grade A, EL 1). The number of punctures should depend on the size of ovary but it should be limited to a maximum of 4–6 (Grade B, EL 4).
- In anovulatory PCOS women with CCR and with no other subfertility factors, who cannot access hospital facility for intensive monitoring, required with gonadotropin therapy or requiring laparoscopic assessment of their pelvis, it is suggested to attempt LOD (Grade C, EL 4).
LOS should not be offered for non-fertility indications, severe male factors, or to women with obstructive tubal disease.
Recommendations on intrauterine insemination
IUI is recommended along with OI in anovulatory sub-fertile PCOS women with associated mild male factor sub-fertility. Also, in anovulatory subfertile PCOS women with unsuccessful conception despite OI, IUI is recommended.
Recommendations for IVF
- IVF is a third-line treatment option in women with PCOS who fail to conceive or who have other indications for IVF. (Grade A, EL 2)
- In anovulatory sub-fertile PCOS women with no other causes of sub-fertility, initiating IVF cycles along with OI is recommended as a third-line treatment option. (Grade C, EL 4)
- In anovulatory sub-fertile PCOS women indicated for IVF, the GnRH antagonist protocol can be suggested over the GnRH agonist long protocol because of reduced incidence of severe OHSS at similar clinical pregnancy rates. (Grade A, EL 2)
Recommendations for luteal phase support
Administration of luteal phase progesterone is recommended in subfertile PCOS women undergoing OI or assisted reproduction. (Grade A, EL 1)
Conclusion
The evolving understanding of PCOS has led to better define this endocrinal disorder. An understanding of the pathology has allowed us to treat the infertile patient more appropriately and improve outcomes.
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author, Dr. Sonia Malik is a Director and HOD Southend Fertility & IVF, New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
