The underrated problem of resistant hypertension and potential treatment options
M3 India Newsdesk Jun 09, 2022
This article explains what is resistant hypertension, how renal denervation is a potential therapy and its relevance in India. The article is also backed up by study findings.
Hypertension (HTN) is the most common and widespread chronic cardiovascular disease in India and around the globe. Using the conventional guideline definition, the long-term prognosis implies that up to fifty per cent of the adult population will suffer from hypertension. The prevalence of resistant hypertension ranges between 8 and 18 per cent of all individuals.
What is resistant hypertension?
Uncontrolled blood pressure (BP) (>140/90 mmHg; >130-139/80-85 mmHg in patients with diabetes mellitus; >130/80 mmHg in chronic kidney disease with proteinuria) despite the use of at least three antihypertensive drugs of different classes, including a diuretic, at maximum, recommended or tolerated dosages.
The most common causes of pseudo resistance include poor adherence, white-coat hypertension, and insufficient medication combination. Based on proper history, this should be distinguished from true resistance. Secondary causes of resistant hypertension should be ruled out by a thorough assessment of these individuals, since they may account for 20% of cases.
There is substantial evidence that the sympathetic nervous system contributes to the formation and progression of almost all phenotypes of HTN. Hence, this has been the focus of novel treatment efforts.
A look at renal sympathetic nervous system pathophysiology
Increased sympathetic nerve activity has been linked to a number of cardiovascular conditions, including hypertension, heart failure, chronic kidney disease, metabolic syndrome, and type 2 diabetes. The sympathetic nervous system delivers efferent (thoraco-lumbar outflow) fibres to the kidneys and receives information for the central nervous system through afferent (mechanoreceptor) fibres.
Renal vasculature, the tubular portion of the nephron, and juxtaglomerular renin-containing granular cells are innervated by efferent fibres. Renin is secreted by the juxtaglomerular apparatus in response to efferent stimulation, which causes tubular salt retention, decreased renal blood flow, and a reduction in renal blood flow. These impacts affect short- and long-term control of blood pressure.
Renal denervation aids in the treatment of drug-resistant hypertension
Renal denervation for hypertension is making a return following a study in 2014. New research shows that it may improve blood pressure (BP) reductions obtained with substantially increased antihypertensive medication in individuals who haven't reacted effectively to first-line medicines.
In the RADIANCE-HTN TRIO study, denervated kidneys successfully reduced blood pressure in individuals who were resistant to at least three hypertension medications administered in combination. Early findings showed both safety and effectiveness for people on various antihypertensives.
The multicenter RADIANCE-HTN TRIO trial involved 989 individuals with hypertension, defined by office blood pressure of 140/90 mm Hg and resistance to at least three antihypertensive medicines, including a diuretic. The participants were transferred to a single tablet comprising a calcium channel blocker, an angiotensin receptor blocker, and a thiazide diuretic, which they were kept on for the duration of the study. Those having a daily ambulatory blood pressure of 135/85 mm Hg or above were randomized to ultrasound-guided renal denervation (n = 69) or a sham treatment (n = 67) after 4 weeks of this standardized treatment. All of the patients had a glomerular filtration rate of at least 40 mL/min/m2.
The great majority of patient's blood pressure was well managed sufficiently with fixed dosage standardized medication that they did not fulfil the study's qualifying requirements. This resulted in a significant drop in the number of individuals randomized, from 989 to merely 136.
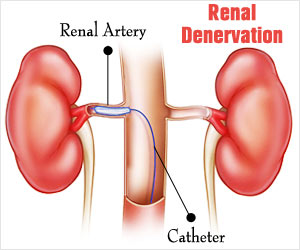
What is renal denervation?
A balloon-based catheter was supplied to the primary renal arteries through percutaneous access during renal denervation. To block renal nerve traffic, a ring of ablative energy was supplied to a depth of 16 mm.
Each primary renal artery received two to three ablative energy lasting seven seconds each, resulting in a circumferential pattern of ablation. Water running via an interior cooling balloon protected the artery wall.
Study findings
The change in daytime ambulatory systolic blood pressure in the intent-to-treat (ITT) group at 2 months was the trial's main objective. Both groups had identical baseline demographic and clinical features, which represented risk factors for resistant hypertension, such as an 82 per cent prevalence of abdominal obesity in both. At screening, the denervation group's office blood pressure was 162/105 mm Hg, while the sham group was 164/103 mm Hg, with patients taking an average of four antihypertensive drugs. The mean daytime ambulatory blood pressure in both groups was around 150/94 mm Hg at the time of randomization.
Three individuals in the renal denervation group and eight in the sham group got extra antihypertensive drugs between baseline and two months. At two months, urine samples revealed that adherence to the combo tablet was above 80%.
Renal denervation lowered daytime ambulatory systolic blood pressure in the ITT group more than the sham treatment from 0 to 2 months, with reductions of 8.0 mm Hg against 3.0 mm Hg. The median difference between groups was 4.5 millimetres of mercury (95 per cent confidence interval 8.5–0.3 millimetres of mercury, adjusted P =.022). The reduction in daytime ambulatory systolic blood pressure in the renal denervation group was 9.7 mm Hg versus 3.0 mm Hg in the sham group, for a median difference of 5.8 mm Hg (95 per cent confidence interval 9.7–1.6 mm Hg, adjusted P =.005) among patients with ambulatory blood pressure data at baseline and follow-up.
Renal denervation reduced 24-hour systolic blood pressure (median difference 4.2 mm Hg, adjusted P =.016), nighttime ambulatory systolic blood pressure (median difference 3.9 mm Hg, P =.044), and office systolic blood pressure (median difference 7.0 mm Hg, P =.037) in the ITT populations, in addition to daytime ambulatory systolic blood pressure When only individuals with ambulatory blood pressure data available at both baseline and follow-up were included, the size of the difference was considerably higher.
In all, 38 per cent of patients who got renal denervation achieved a daytime ambulatory blood pressure of less than 135/85 mm Hg (P =.031), compared to just 21% of controls.
Adverse events
In terms of adverse events, one access site pseudoaneurysm in the renal denervation group was effectively treated. At two months, there was no renal artery stenosis and no change in renal function across groups.
Dr. Kirtane, lead investigator opined:
“In patients with resistant hypertension to guideline-recommended triple combination therapy in a single pill, ultrasound-guided renal denervation was associated with an 8.0 mm Hg reduction in daytime ambulatory systolic blood pressure, which is 4.5 mm Hg greater than a sham procedure. Renal denervation had a stronger blood pressure reducing impact than sham for 24-hour, nocturnal, and office systolic blood pressure."
These findings are similar to those of RADIANCE HTN SOLO. Longer-term studies are needed and are continuing at present moment in individuals with mild-to-moderate hypertension, indicating that ultrasound-guided renal denervation can drop blood pressure throughout a range of hypertension.
Relevance for India
A secondary-care practice in India has a high prevalence of resistant hypertension. It is much higher in women and elderly people. It's vital to note that the resistant hypertension sea begins when the secondary HTN coastline is reached and the resistant hypertension island is still unexplored. Resistant hypertension is a new trait, and there's mounting evidence that these people exhibit sympathetic hyperactivity. The role of the novel Renal Denervation, on the other hand, is to show encouraging outcomes. Hypertension is a serious concern in India, and governmental agencies must produce guidelines for the best BP management measures at the clinical and community levels in order to lessen the country's growing burden.
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
The author is a practising super specialist from New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
