Simplified in Practice: ECG nuggets for atrioventricular block of the first degree
M3 India Newsdesk Mar 17, 2022
In this segment of Simplified in Practice, we will focus on the atrioventricular block of first degree and discuss the factors leading to it, along with its clinical significance.
First-degree atrioventricular node block
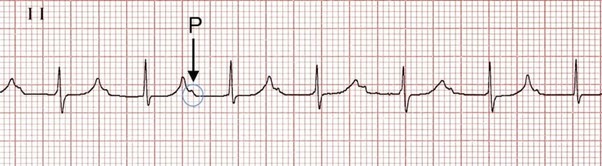
Conduction via the AV node is delayed with a first-degree atrioventricular node block, prolonging the time it takes for the action potential to travel from the sinoatrial node through the AV node and into the ventricles. A prolonged PR interval on the ECG indicates a first-degree AV block.
It is important to remember that the P wave is a sign of atrial depolarisation that is triggered by a firing of the SA node. The atrial depolarisation finally extends to the AV node, where the electrical impulse is delayed somewhat before reaching the ventricles. The impulse will take longer to reach the ventricles if the AV nodal conduction (dromotropy) is reduced, resulting in a wider gap between the P wave and the QRS complex. The PR interval will be lengthened because the QRS complex suggests ventricular depolarisation.
Criteria
PR interval > 200ms (five small squares)
Conduction from the atria to the ventricles is delayed but not interrupted.
If the PR interval is more than 300ms, there is a marked first-degree heart block
In most cases, the PR interval is between 0.12 and 0.20 seconds. A first-degree AV block is indicated by a PR interval that is regularly longer than 0.20 seconds or five tiny boxes. In the first-degree AV block, the ratio of P waves to QRS complexes is 1:1, as opposed to the second-degree, or 2nd degree, and third-degree, or 3rd degree, AV nodal blocks.
Factors causing first-degree heart block
First-degree heart block may be caused by a variety of factors like:
- Athletic training
- Increased vagal tone
- Inferior MI
- AV nodal blocking medicines (beta-blockers, calcium channel blockers, digoxin, amiodarone)
- Myocarditis (e.g. Lyme disease)
- Electrolyte problems (e.g. Hyperkalaemia)
- May be a normal variety
Clinical significance
- It is not dangerous when this is found on its own. It does not cause haemodynamic instability when it is found alone.
- There is no need for special therapy. A first-degree AV block is, in general, a harmless condition that does not need therapy. It may, however, be a sign of future higher-degree AV block, and AV blocking drugs may be avoided depending on the PR interval.
AV blockages on ECG in a simple manner:
*p wave = wife*
*qrs complex = husband*
*Pacer = counselling*
Sinus Rhythm (Normal)
- The wife (p wave) is waiting for her husband at home (qrs)
- Every night, the spouse (qrs) arrives on schedule
AV block of the first degree
- At home, the wife (p wave) is waiting
- The spouse (qrs) arrives late every night, but he does so consistently and at the same time each night
Type I (Weinkebach) 2nd degree block
- At home, the wife (p wave) is waiting
- Every night, the spouse (qrs) arrives later and later till one night he does not arrive at all
(Note: to notice this trend, the spouse (qrs) must return home for at least two evenings in a succession.)
AV block type II, 2nd degree
- At home, the wife (p wave) is waiting
- Occasionally, the spouse (qrs) returns home, and occasionally, he does not. When he does return home, he always does so at the same time
(Note that this is often more significant than type I (Weinkebach) and may need therapy) (pacer).
AV block of the 3rd degree
- The wife (p wave) is no longer at home waiting for her husband.
- She and her husband (qrs) are now on different schedules, have no connection, and no longer communicate. Each partner has his or her own timetable.
(It's worth noting that this typically necessitates counselling in the form of a temporary or permanent pacemaker.)
This is the next part of our series- Simplified in Practice where we break down ECG interpretation for various conditions. To read the earlier parts of the series, click here: Simplified in Practice: ECG basics & how to interpret, Simplified in Practice: How to detect myocardial ischaemia?, Simplified in Practice: Anterior Myocardial Infarction- Clinical nuggets on ECG characteristics, Simplified in Practice: What are the ECG changes when inferior STEMI starts?, Simplified in Practice: ECG features of posterior MI Simplified in Practice: ECG nuggets in old STEMI (LV aneurysm, Simplified in practice: ECG Nuggets for atrial flutter, & Simplified in practice: Understanding ECG features of ectopic heartbeats
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author is a practising super specialist from New Delhi.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
