Pulpectomy in Paediatric Patients
M3 India Newsdesk Jul 30, 2024
The article explains pulpectomy in primary teeth, covering its goals, indications, contraindications, diagnostic criteria, procedural steps, and materials used for obturation. It highlights the specifics of partial and total pulpectomy and the required armamentarium.
Mathewson (1995) defined it as the complete removal of necrotic pulp from the root canals of primary teeth and filling them with an inert resorbable material to maintain the tooth in the dental arch.
Goals of pulp therapy in primary/mixed dentition
- Successful management of the curiously involved pulp
- Maintenance of arch length and tooth space
- Restoration of comfort with the ability to chew
- Prevention of speech abnormalities and abnormal habit
Indications
- Traumatised primary incisors with resultant pathologic conditions (in children younger than 4 to 4.5 years.
- Tooth with irreversible pulpitis or a necrotic pulp.
- Excessive haemorrhage (hyperaemia) during pulpotomy procedure.
- Carious primary teeth with the presence of draining sinus tracts or intraoral/extraoral swelling.
- No evidence of pathologic root resorption of more than two-thirds or a fourth of root length.

What are the Contraindications
Clinical contraindications:
- Tooth which is not restorable.
- Insufficient tooth structure to allow isolation by a rubber dam.
- Chronic illness with leukaemia, rheumatic and congenital heart disease, chronic kidney disease, etc.
- Excessive tooth mobility.
- Communication between the oral cavity and area of furcation.
- Communication between the floor of the pulp chamber and the region of furcation.
Radiographic contraindications
- External root resorption with less than two-thirds of primary root structures remaining.
- Within root resorption at the root's apical third.
- In the case of radicular cyst.
- Intraradicular radiolucency that communicates with the gingival sulcus.
- Pathologic condition extending to developing permanent tooth bud.
Diagnostic criteria for pulpectomy
- History of pain
- Severe toothache at night
- Spontaneous, long-lasting pain
Clinical signs and symptoms
- Gingival abscess- Associated with a tooth with a deep carious lesion
- Draining fistula- Associated with a tooth with a deep carious lesion
- Extraoral swelling- Associated with a tooth with a deep carious lesion
- Abnormal tooth mobility
Types of pulpectomy
Partial Pulpectomy and Total Pulpectomy
1. Partial pulpectomy
- When the pulp is vital but shows clinical evidence of hyperaemia
- No suppuration
- No radiographic evidence of thickened PDL or radicular disease
2. Total pulpectomy
Single visit pulpectomy
It is carried out as an extension of the pulpotomy procedure.
Steps :
- Identification of root canals
- Determining working length
- Removal of all pulpal tissue
- Drying of canals
- Application of formocresol for 5 minutes
- Obturation
- Restoration of tooth
Two visit pulpectomy
- 1st visit – Removal of pulp.
- 2nd visit – remaining contents of the canal are removed.
- If asymptomatic – canals are filled with obturating material.
- Painful tooth/moisture in canals – canals are mechanically cleaned again.
Armamentarium
- Local anaesthesia
- Rubber Dam
- Access Opening Burs
- Basic Endodontic Instruments
- Reamers
- Broaches
- Files – H-files| K-files| Ni-Ti files
Steps in pulpectomy
1. Access opening
- All caries were removed with a slow-speed round bur/ spoon excavator
- From the point of pulp exposure, access is established by connecting pulp horns with bur
- Straight line access
2. Determination of Working Length (WL)
“The distance from the coronal reference point to the point at which canal preparation and obturation should terminate.” – Glossary of Endodontic Terms.
3. Bio-mechanical preparation (BMP) and chemo-mechanical preparation
Instrument movements while shaping.
- Watch-winding
- Reaming
- Filing
- Rotary
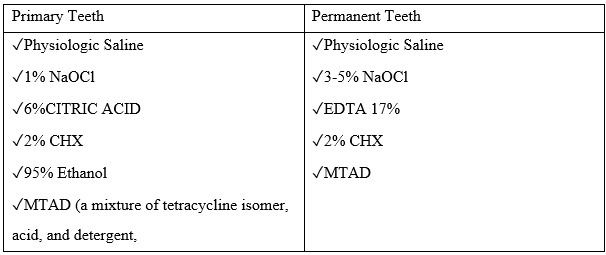
Root canal irrigation in pediatric endodontics.
- Facilitate removal of necrotic tissue and dentin chips
- Avoid putting contaminated soft and hard tissue into the periapical region and the root canal apically.
- Dissolve organic and/or inorganic tissue
- Exhibit antimicrobial activity
Recommended Irrigants:
4. Obturation in primary teeth
Aim - is to prevent recontamination of canal from either apical or coronal leakage and to isolate and neutralise any remaining pulpal tissue or bacteria.
Materials used for obturation are :
- Zinc oxide eugenol (ZOE)
- For primary teeth, the initial recommended material for a root canal filling
- Described by Sweet in 1930
Composition :

It provides a sedative effect in deep preparations so, it remains as the material of choice for pulpotomies or pulpectomies in primary dentition.
- Calcium hydroxide
- Introduced by Herman
- Has pH >12
It is initially bactericidal then bacteriostatic, promotes healing and repair, has a high alkaline pH that stimulates fibroblasts, stops internal resorption, and is inexpensive and easy to use.
The main disadvantage it tends to resorb earlier than physiological resorption.
- Iodoform
Iodoform-based paste are - KRI paste, Maisto paste, Guedes-Pinto paste, Rifocort, Endoflas, Vitapex/Metapex.
- Walkhoff Paste
- Introduced by Walkhoff in 1928
- Consists of iodoform, parachlorophenol 33-37%, camphor – 63-67% and menthol
- KRI Paste
- Introduced by Volkoff
- Consists of Iodoform (80.8%), camphor (4.86%), para chlorophenol (2.025%), and menthol (1.215%)
- Maisto’s Paste- By Maisto - 1967.
Consists of zinc oxide -14 g, Iodoform-42 g, thymol -2 g, Chlorophenol camphor -3 cc, lanolin – 0.5 g.
- Guedes-Pinto Paste
By Guedes-Pinto in 1981 composed of Rifocort, camphorated para chlorophenol and Iodoform.
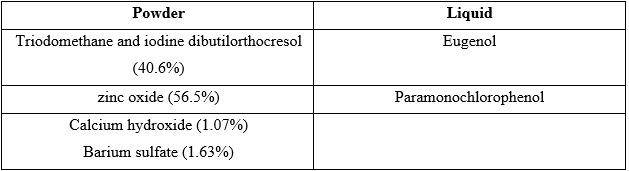
- Endoflas
Endoflas is a resorbable paste containing components similar to that of Vitapex, with an addition of Zinc oxide eugenol.
- Vitapex/Metapex
By Kawakami et al. - 1979
It is a syringe-loaded viscous pre-mixed paste composed of Iodoform - 40.4%, Calcium hydroxide - 30.3%, Silicone oil- 22.4% and others – 6.9.
- Chitra HAP-Fil
It is a hydroxyapatite nanoparticle gel-based root filler material, which exactly corresponds to the mineral content of bone and dentin.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Neha Kalantri is a practising dentist from Nashik.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
