Perinatal & Infant Oral Health Care
M3 India Newsdesk Jun 25, 2024
The article explains the importance of early oral health habits in infancy, including prenatal care, proper diet, and early dental visits, to prevent future dental issues. It also provides recommendations for parents on maintaining their child's oral health and managing common oral conditions.
The American Academy of Pediatric Dentistry (AAPD) acknowledges that to improve a child's chances of living a lifetime free from preventable oral illness, preventative education and dental care must be built upon the foundations of perinatal and infant oral health.
Oral health and infant (defined as children under the age of twelve months) may not seem like terms that go together at first. After all, the majority of newborns are born toothless and often remain that way for the first six months of their lives.
Babies most likely have a small number of teeth by the time they become one year old. Why even bother about oral health in infancy, one would wonder? It turns out that an individual's oral health as well as general health and well-being into adolescence and beyond can be impacted by the behaviors they form during infancy, both positive and negative ones.
Why even bother about oral health in infancy, one would wonder? It turns out that an individual's oral health as well as general health and well-being into adolescence and beyond can be impacted by the behaviors they form during infancy, both positive and negative ones.
Pregnancy and perinatal period
Pregnant women's health and the health and well-being of their newborn infants are greatly influenced by the perinatal period.
Offspring's dental health is positively correlated with the oral health of their mothers. Prenatal dental education and preventative treatments are effective in lowering the incidence of Mutans streptococci (MS) in children, according to a comprehensive review.
Certain drugs may be dangerous for women and men who are capable of becoming pregnant, nursing mothers, and perinatal infants. Current U.S. Food and Drug Administration (FDA) recommendations can assist healthcare providers when using in-office, prescribed, and over-the-counter medications for these individuals.
Common oral conditions are listed in the table below. While the FDA advised against dental amalgam use in 2020 for children under the age of six, women who are nursing, and women who are pregnant or want to become pregnant, it is important to emphasize that dental visits during pregnancy are safe, and effective, and should be encouraged.
Diet for newborns and infants
The benefits of breastfeeding in a child’s first year of life are clear. However, breastfeeding and baby bottles beyond 12 months, especially if frequent and/or nocturnal, are associated with early childhood caries (ECC).
juice in a bottle, package, open cup, or travel-sized covered cup should not be given to children throughout the day.
It's important to remember that consuming free sugars on a regular basis—that is, sugars that are naturally found in honey, syrups, fruit juices, and fruit juice concentrates—also accelerates the carious process.
The American Heart Association recommends that sugar in foods and drinks be avoided by children under two years. Additionally, the American Academy of Pediatrics recommends that 100 per cent fruit juice not be introduced before 12 months of age and be limited to no more than four ounces a day for kids between the ages of 1 and 3 years.
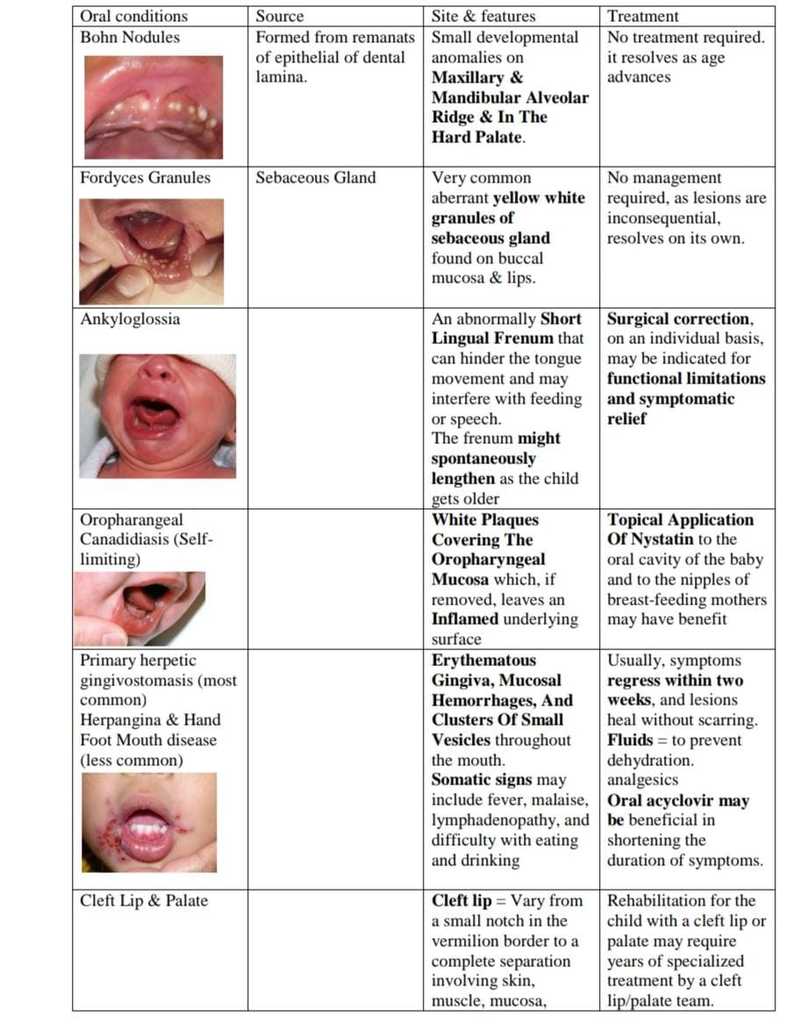
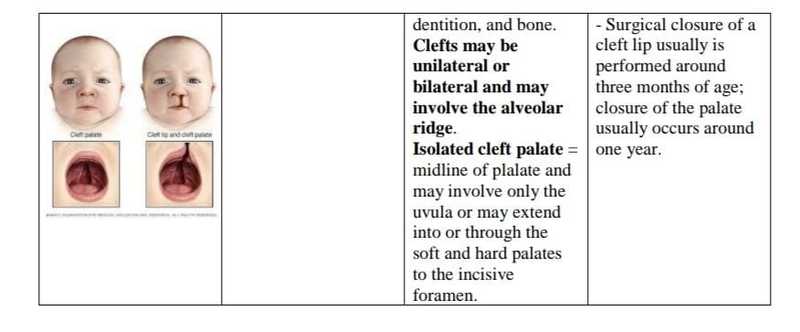
Common oral conditions
Dental eruption (Teething)
- While neonatal teeth erupt during the first month of life, natal teeth are present at birth. Neonatal or baby teeth can cause discomfort for mothers due to biting or abrasion of the breast during nursing, as well as occasional soreness and unwillingness to feed.
- Riga-Fede illness is the result of the tongue repeatedly rubbing against a baby tooth when swallowing and moving, causing ulceration, bleeding, and discomfort. It might be necessary to extract the tooth if it is movable and there is a risk of it being detached and aspirated.
- Decisions regarding the extraction of prematurely erupted primary teeth and smoothing the incisal edge should be made on an individual basis.
- While many children appear to have no problems, sporadic localised discomfort, agitation, low-grade fever, and excessive salivation might result from teeth eruption, or teething.
The use of topical anaesthetic or homoeopathic remedies to relieve discomfort should be avoided due to the potential harm of these products in infants. Because of the risk of methemoglobinemia, benzocaine use is contraindicated in children younger than two years of age.
Dental caries risk in newborns and infants
Any primary tooth in a kid younger than six years old that has one or more decaying (non-cavitated or cavitated lesions), missing, or filled (owing to caries) surfaces is referred to as having early childhood caries (ECC). Similar to other types of caries, phasic demineralisation and remineralisation of dental hard tissues are the outcomes of ECC, a complex, dynamic disease driven by bacteria and sugar.
Traditional microbial risk markers for ECC include acidogenic-aciduric bacterial species, namely MS and Lactobacillus species. MS may be transmitted vertically from caregiver to child through salivary contact, affected by the frequency and amount of exposure.
Additionally, there is horizontal transmission, which can happen between daycare children or other family members. Primary teeth dental caries can cause long-term discomfort, infections, and other health problems.
ECC has a major impact on the quality of life of children and their families and is an unnecessary health and financial burden to society. dentition, and bone.
Prevention for ECC needs to begin in infancy. Due to their frequent interactions with the family throughout the child's first year of life, doctors, nurses, and other healthcare professionals may have more opportunities to teach the parent or caregiver than dentists.
As a result, they must be knowledgeable about the risk and protective factors for dental caries and utilise this knowledge to spread primary care preventive messages that include:
- Limiting sugar intake in foods and drinks
- Avoiding night-time bottle feeding with milk or drinks containing sugars
- Voiding baby bottle usage and breastfeeding beyond 12 months, especially if frequent and/or nocturnal
- Have the child’s teeth brushed twice daily with a smear of fluoridated toothpaste
Additionally, for children who are at high risk for dental caries, professionally applied fluoride varnish and dietary fluoride supplements (for infants living in non-fluoridated areas) may be part of an individualised preventive plan. However, a growing number of caregivers are hesitant about professionally-applied topical fluorides.
Fluoride hesitancy mirrors vaccination hesitancy observed in pediatric medicine. Inaccurate information about fluoride may be shared among caregivers within online social networks.
Recommendations
1. Advise expecting and new parents regarding the importance of their oral health and the possible transmission of cariogenic bacteria from the parent/ primary caregiver to the infant.
2. Encourage the establishment of a dental home that includes medical history, dental examination, risk assessment, and anticipatory guidance for infants by 12 months of age.
3. Provide caries preventive information regarding the high frequency of sugar consumption; brushing twice daily with an optimal amount of fluoridated toothpaste; safety and efficacy of optimally fluoridated community water; and, for children at risk for dental caries, fluoride varnish and dietary fluoride supplements (if not consuming optimally fluoridated water).
4. As the primary dentition starts to erupt, determine the caries risk to allow the proper preventative strategies.
5. Inform parents about frequent oral health issues that affect newborns and infants, nonnutritive oral behaviours (such as sucking fingers, using pacifiers), teething (which involves using analgesics and avoiding topical anaesthetics), growth and development, and orofacial trauma (including play objects, pacifiers, car seats, electric cords, and falls when learning to
walk).
6. When ankyloglossia results in functional limitations or causes symptoms, the need for surgical intervention should be assessed on an individual basis.
7. When a patient presents with a prematurely erupted primary tooth (i.e., natal or neonatal tooth), decisions regarding intervention should be individualised, based on the interference with feeding, the risk of detachment and aspiration, and any medical or contributing considerations.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Pallavi Jhawar, MDS - Pedodontics and Preventive Dentistry, Consultant Shri Zawar Dental Clinic, Jalna.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
