Snoring can Disturb More than Sleep! Understanding Obstructive Sleep Apnoea (OSA)
M3 India Newsdesk Sep 09, 2022
This article advises physicians on how to diagnose and treat Obstructive Sleep Apnoea (OSA) and how proper measures can avert some significant complications and can increase the life expectancy and quality of life for an individual.
We often hear spouses complaining about losing sleep because of their better half and their loud grumbling and snoring sounds. Most of them treat it like any other common issue and let go but habitual loud snoring can be indicative of something serious. And if left untreated, it can lead to some serious debilitating health conditions and can also subsequently reduce the life expectancy of the person.
Understanding OSA
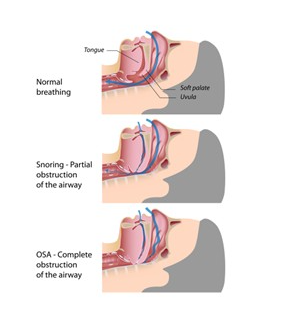
Obstructive sleep apnoea is a sleep disorder in which repetitive episodes of nocturnal cessation of breathing occur. This is due to the collapse of the upper respiratory tract. It is a chronic condition and affects around 2-4% of the adult population with the highest prevalence among middle-aged men. These obstructive episodes can cause progressive asphyxia that stimulates the breathing efforts against the collapsed airway.
Prevalence and incidence of OSA
In the general population, OSA affects approximately 4% of middle-aged men & 2% of middle-aged women. On the basis of average prevalence, it is estimated that 1 in 5 individuals will have Mild OSA whereas 1 in 15 will have moderate OSA.
Gender prevalence
Males are at a higher risk of developing OSA as compared to females. There are a few studies which have proposed different theories to support this fact. An investigator found out that the total neck soft tissue volume was significantly greater in males as compared to females and this increased volume can be a reasonable cause of an enlargement of the soft tissues of the upper airway creating a narrower airway and predisposing the subject to OSA.
Another interesting theory is about the genioglossus muscle. Women show increased activity of this muscle in the state of wakefulness, leading to greater upper airway stability Also the female hormones (possibly progesterone) have shown a great impact on this muscle. If this cumulatively augmented muscle activity continues even during sleep, the chances of the upper airway collapsing are less.
Mechanism of occurrence of OSA
- Distinguishing between these two important terms, the term apnoea means complete cessation of breathing while hypopnoea means a partial stoppage of breathing.
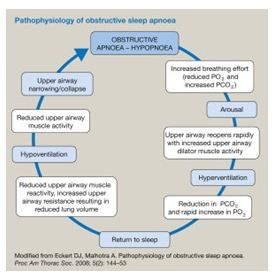
- The cycle of developing an episode of either apnoea or hypopnoea lies between the initiation of sleep, arousal from sleep and returning back to it.
- There are episodes of hypoventilation leading to a reduced upper airway muscle activity causing the consequent collapsing of the airway.
- Following the collapse, there will be an increased breathing effort which causes arousal from sleep leading to increased activity by the upper airway dilator muscle causing a state of hyperventilation and post that the person suffering from OSA will go back to sleep.
- This cycle continues nocturnally leading to some nocturnal signs and symptoms and a few diurnal too.
Risk factors and causes of OSA
- Excessive weight (Obesity)
- Thicker neck (More neck circumference can be a cause of a narrower airway)
- An obstructive airway (Tonsils or adenoid enlargement)
- Prolonges nasal congestion
- Males are more prone to developing OSA as compared to females
- Older adults (The chances of OSA increase with age)
- Smoking, alcohol, sedatives and Tranquilizers
- Medical co-morbidities like Congestive heart failure, Hypertension, Type 2 diabetes mellitus, chronic lung disease, Parkinson's disease etc.
Symptoms and clinical features of OSA
A few patients suffering from OSA show significant and noticeable signs whereas a few never develop any noticeable symptoms or a few might attribute it to another cause. Symptoms are present at both night and daytime and can interfere with the person’s day-to-day activities.
Symptoms occurring at night time
- Loud snoring
- Sudden snorting, gasping or a feeling of choking during sleep
- Mouth breathing with sleeping
- Discomfort during sleep leads to constant tossing and turning
- The urgency to urinate
Symptoms occurring at day time
- Daytime sleepiness
- Fatigue throughout the day
- Waking up with a feeling of tiredness
- Morning headaches
- Dry mouth in waking up
- Loss of memory
- Decreased libido
Medical complications due to OSA
This sleeping disorder predisposes patients to many other medical co-morbidities like
- Cardiovascular disorders (CVD)
- Hypertension
- Type-2 Diabetes Mellitus
- Non-alcoholic fatty liver
- Metabolic syndrome
- Mental health disorders
The prevalence of cardiovascular disorders is 40-60% more in patients with OSA as compared to other medically healthy patients. Furthermore, this prevalence has increased over the past two decades by a whopping 30% and this can be simply attributed to an obesity pandemic and deleterious lifestyle changes. It is also said that patients with heart failure sleep approximately 1.5 hours less than normal patients.
Why are patients with OSA more prone to heart failure (HF)?
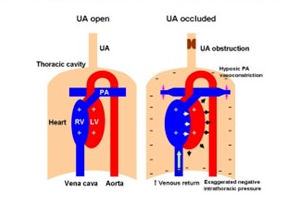
- OSA is characterised by a typical upper respiratory tract obstruction.
- This increases the left ventricular (LV) transmural pressure leading to negative intrathoracic pressure and thus increases the afterload.
- It also increases the venous return and right ventricular (RV) pre-load and leads to OSA-induced hypoxic Pulmonary Artery (PA) vasoconstriction which increases the RV afterload.
- A combination of increased LV afterload and decreased preload reduced the cardiac output and stroke volume, thus making the patient more prone to HF.
Diagnosis of OSA
The following parameters can be used for diagnosing OSA:
- History taking (The Epworth Sleepiness Scale (ESS) questionnaire is commonly used)
- Physical examination
(Body mass index above 30 kg/m2, Modified Mallampati score of 3 and 4 and large neck circumference above 17 inches in men or 16 inches in females, elevated blood pressure, signs of pulmonary arterial hypertension).
- STOP-BANG questionnaire
- Polysomnography (Sleep test)
Through this test OSA has confirmed if either of the following two conditions exists:
- There are 15 or more episodes of apnoea, hypopnoea or respiratory arousals per hour of sleep in an asymptomatic patient. More than 75% of them must be obstructive.
- There are more than 5 or more episodes of apnoea, hypopnoea or respiratory arousals per hour of sleep in a patient with disturbed sleep. More than 75% of them must be obstructive.
Treatment for OSA
- Positive Airway Pressure like Continuous Positive Airway Pressure (CPAP) and Bilevel Positive Airway Pressure (BPAP)
- Oral devices like Mandibular Advancement Device (MAD) and Tongue retaining device
- Surgical procedures like Jaw surgery or Uvulopalatopharyngoplasty (UPPP)
- Upper airway stimulation
- Weight loss
- Lifestyle modification
Click here to see references
Disclaimer- The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Ridima Surve is a practising dentist from Mumbai.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
