Minimally Invasive Dentistry
M3 India Newsdesk Dec 23, 2024
A patient-centred approach to dental care, Minimally Invasive Dentistry MID seeks to maintain long-term oral health and retain healthy tooth structure. This article explains the principles and applications of minimally invasive dentistry.
Minimal Invasive Dentistry MID
- Dr. G. V. Black, the father of modern dentistry.
- Cavity designs were classified and standardised-1891.
- Sound tooth structure was sacrificed for geometric perfection and to accommodate the shortcomings of restorative materials.
- ‘Extension For Prevention’.

- It was G J Mount 1991 who first cited the need for ‘Minimal Treatment’ of dental caries.
- Davis and Makinson 1992, first termed ‘Minimal Intervention Dentistry’ in the literature.
Definition
Minimum intervention dentistry (MI) can be defined as a philosophy of professional care concerned with the first occurrence, early detection and earliest possible cure of disease on micro levels, followed by minimally invasive, patient-friendly treatment to repair irreversible damage caused by such disease.
Differences between Minimal Intervention Dentistry, Minimally Invasive Dentistry and Micro-Dentistry
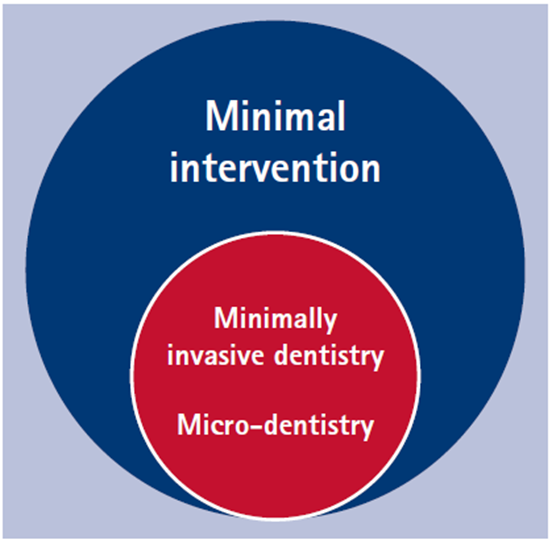
- This is a diagram illustrating how minimal intervention dentistry and minimal invasion (minimally invasive dentistry) are not interchangeable terms.
- Minimally invasive dentistry is a phase of minimal intervention.
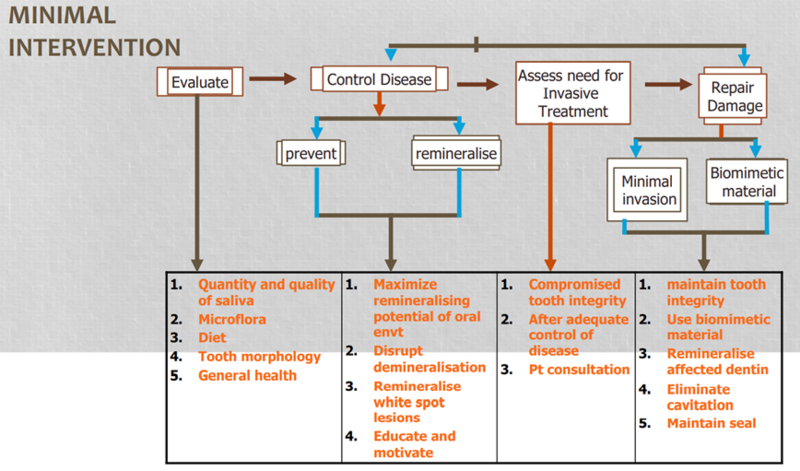
Strategies of MID: Dawson and Makison (1992)
Principles of MID
- Early caries diagnosis.
- Classification of caries depth and progression.
- Assessment of individual risk.
- Optimal caries preventive measures.
- Remineralisation of early lesions.
- Minimal surgical intervention of caries lesions.
- Repair rather than a replacement of defective restoration.
- Assess disease management outcomes at intervals.
1. Early caries diagnosis
A. Initial carious lesion
- The purpose of the examination is to detect visual changes in colour, translucency and structure of the enamel.
- Cavities and brown or white stains can be found with a first examination, tooth by tooth, on wet surfaces. Initial examinations may also be performed to assess periodontal health and restorations.
- At this point, the accumulation of plaque biofilm and gingival pathology at suspected sites must be examined in order to assess caries activity.
- With light pressure, a blunt or rounded probe (a periodontal probe is suitable) can be employed.
- The following clinical parameters show and measure the activity state of a single carious lesion:
- The lesion's severity was connected with how it looked.
- The lesion's location (whether it is in a region that encourages plaque accumulation or not).
- Tactile perceptions when probing (used to evaluate the enamel's roughness and the presence of surface deposits).
- The status of the gingival margin concerning the areas of interest (evaluated by the absence or presence of bleeding caused by careful probing).
B. Extensive clinical observation
- Changes in colour and translucency that indicate the state of demineralisation should be noted.
- The International Caries Detection and Assessment System (ICDAS) is a classification system that rationalises these outward indicators of dental caries.
- The classification includes six codes. Initial lesions are mainly covered by Codes 1 and 2.
- ICDAS II Code 0: The tooth is healthy.
- ICDAS II Code 1: The tooth has a lesion visible only after drying and histology reveals that the lesion is limited to the external half of the enamel.
- ICDAS II Code 2: The lesion penetrates the full thickness of the enamel. Clinically, an opacity or discolouration distinctly visible without air-drying is apparent but without cavitation.
New diagnostic aids
There are various recent diagnostic aids such as electrical conductance measurement, quantitative light-induced fluorescence, dye-enhanced laser fluorescence, diagnodent, fibre optic trans illumination, digital radiology, digital subtraction radiography, optical coherence tomography. Early caries detection can be achieved with electrical impedance tomography and tunable aperture computed tomography.
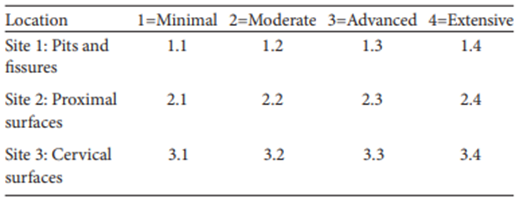
2. Classification of caries depth and progression:
- Classification based on site and size of the lesion.
- In 1997, Mount and Hume developed a new division of the carious lesion.
- Proper access to the lesions, which are infected and broken down to the point where remineralisation is no longer possible, was the main aim behind this classification. The classification is linked to the stage of progression of the lesion and is not related to cavity design.
3. Assessment of individual risk
- Risk is the likelihood that something negative may happen. Caries risk is defined as “the probability of future caries disease development.”
- American Academy of Pediatric Dentistry recognises that caries-risk assessment and management protocols can assist clinicians with decisions regarding treatment and are essential elements of contemporary clinical care for infants, children, and adolescents.
- Identification of caries risk at an early stage can be done by recording patient history, clinical examination, nutritional analysis, and salivary analysis and by using accurate caries diagnostic methodologies.
- Risk assessment
- Encourages the management of the illness's course rather than its result.
- Helps to personalise preventive conversations and provides insight into the illness factors for a particular patient.
- Individualises selects and determines the frequency of preventive and restorative treatment for a patient.
4. Optimal caries preventive measures
- Diet counselling and sugar substitutes
- Pits and fissure sealants
- Antimicrobial agents and chemotherapeutic approaches
5. Remineralisation of early lesions
Remineralisation delivery methods materials include toothpaste, mouth rinses, gels, pastes, chewing gums, lozenges, foods, and beverages.
6. Minimal surgical intervention of carious lesions
The principles of minimally invasive restoration are:
- The shape of the cavity is dictated by the caries and is unique for each carious lesion (conservative cavity preparation).
- Only demineralised enamel and infected dentine are removed, and affected dentine can be left.
- Micromechanical retention is not required.
- Undermined enamel cavities can be restored with adhesive materials.
Because adhesive materials don't require the addition of mechanical retention elements, tooth structure can be preserved with minimum invasive cavity preparations.
Biomimetic potential including the release of fluoride, calcium and phosphate ions can be of value in enhancing remineralisation potential of the carious lesion. GIC, composites, and other materials are among the materials that can be utilised.
a. Atraumatic restorative treatment (ART)
b. Chemo-mechanical method of caries removal
Advantages of chemomechanical caries removal
- Its proven effectiveness
- Method’s safety
- Elimination of local anaesthesia and bur
- Lower anxiety built in patients
- Conservation of the sound tissue
- Only demineralised dentin containing denatured collagen is affected
- Gel consistency lowers the chance of spills and makes application control easier
A. Caridex system
- Caridex solution I – Sodium hypochlorite.
- Caridex solution II – Glycine, aminobutyric acid, sodium hydroxide, sodium chloride.
- Basis – Based on the softening effect of NMAB - N-monochloro-DL-2-aminobutyrate (NMABsystem).
- Delivery system – Consists of a reservoir that stores the solution, a pump with a heater that warms the reagent to body temperature and pushes it through a tube, which is delivered through an applicator tip.
- Delivery mode:
- The two solutions are mixed just before use; it forms a working reagent at a pH of 11 which is stable for 1 hour.
- The solution is applied with an applicator tip which comes in various sizes/shapes.
- Mechanical excavation
- The softened dentin is gently excavated by excavators and removed by aspiration.
- In a moderately sized cavity, it takes roughly five to ten minutes to reach sound dentin.
- Merits
- Avoids painful removal of carious dentin.
- Eliminates the requirement of anaesthetic administration.
- Leaves sound dentin untouched.
- Demerits
- It eliminates the complete carious dentin, including the turbid or diseased dentin as well as the afflicted dentin.
- If sound dentin is attained, it leaves a scaly surface with undercuts and overhangs that cannot be objectively determined (there is no colour code for indication).
B. Carisolv
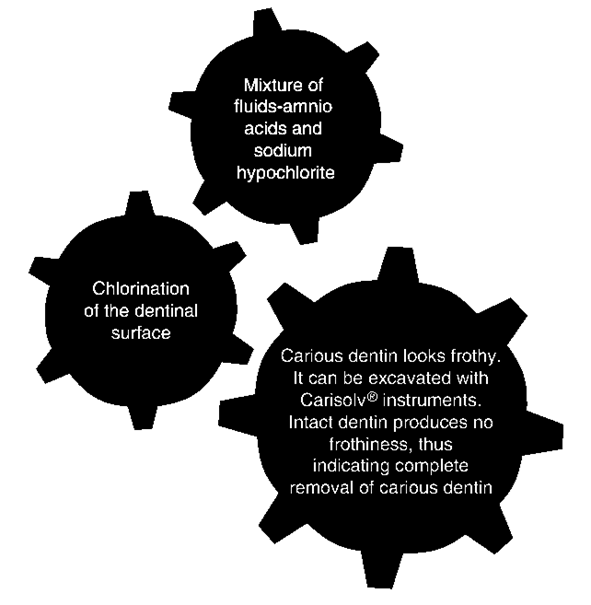
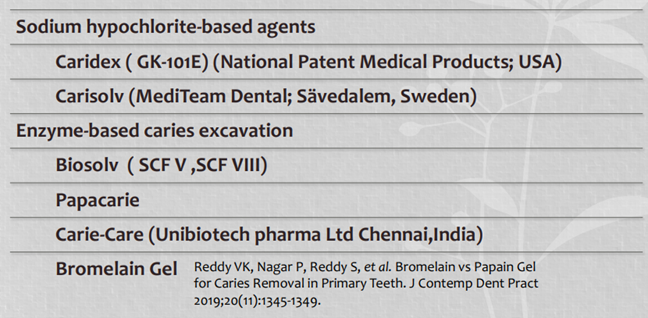
A Systematic Review and Meta-Analysis of Randomised Clinical Trials on Chemomechanical Caries Removal by Hamama et al in 2015 found that the current scientific evidence shows that the sodium hypochlorite-based. Comparing the enzyme-based (Papacarie) chemomechanical and conventional caries eradication procedures, the Carisolv chemomechanical method took longer.
C. Air-abrasion excavation
- In order to remove tissue, the incident particles' kinetic energy must be transferred to the softened dentine surface at a high speed.
- It is an alternative means of cavity preparation by providing a truly conservative preparation for the preservation of a maximal sound tooth structure.
- Bonded restorations combined with air abrasion dentistry provide truly minimal intervention dentistry.
D. Excavation by sonic abrasion
The Cariex system (Kavo Dental; Biberach, Germany)
E. Laser excavation
The erbium-loaded yttrium-aluminium-garnet (Er: YAG) and the erbium, chromium: yttrium-scandium-gallium-garnet (Er, Cr: YSGG)
- According to reports, lasers can eliminate mutans streptococci and remove hard tissue while selectively removing cavities, leaving behind healthy enamel and dentine.
- It has various advantages i.e. selectively removes caries, seals dentinal tubules to reduce sensitivity, is well tolerated by pediatric patients, does not need LA, does not leave a smear and better bonding and conservation of tooth structure can be done.
F. Fluorescence-aided Caries Excavation (“FACE”)
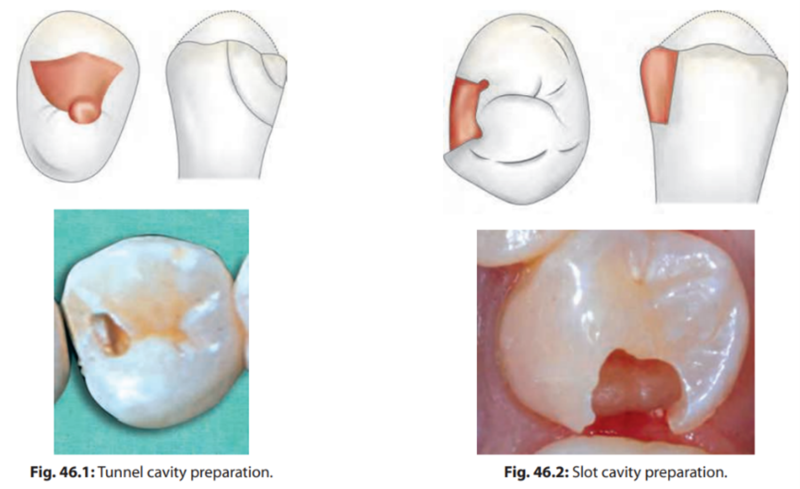
G. Designs of cavity preparations
- Tunnel preparations / Open/Close/Partial/Blind
- Box only preparations
- Slot or Minibox cavity Preparations
- Saucer preparations
- Microchip cavity preparation
- Full box cavity preparation
H. Modifications in the burs
- Fissurotomy bur: Micro STF and Micro NTF versions of the original.
- Micro Diamond Prep System (Brasseler USA): Set of eight burs.
- SMART BURS, or Polymer Caries Removal Burs, are slow-speed rotating handpieces that rotate between 500 and 800 rpm.
Ceramic burs: The CeraBurs (Komet-Brasseler; Lemgo, Germany) are all-ceramic round burs made of alumina-yttria stabilised zirconia and are available in different diameter sizes.
I. Hall technique - A new method
A prefabricated metal crown is cemented over cavitated tooth, using a low-viscosity GI. This crown is placed only after removing debris but without the removal of decomposed carious dentine.
7. Repair rather than replacement of defective restoration
- According to clinical research, removing an existing restoration would result in the loss of a substantial amount of good tooth structure, which will lead to the need for larger dental restorations.
- The decision to repair rather than replace a restoration always must be based on the patient’s risk of developing caries, a conservative approach to repair and a professional’s judgment of benefit versus risk.
8. Assess disease management outcomes at intervals
Recall at various intervals should be done to reduce the recurrence of caries.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Neha Kalantri is a practising dentist from Nashik.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
