How to: Assessing an overactive thyroid & planning treatment- Dr. SK Wangnoo
M3 India Newsdesk Feb 15, 2021
The assessment for overactive thyroid gland is directed towards identifying whether the patient is having thyroiditis – which is usually self-limiting and needs only symptomatic treatment or requires definitive management for hyperthyroidism. This is assessed by doing appropriate laboratory radiographic assessment which is prompted by features suggestive of overactive thyroid gland. Dr. SK Wangnoo as part of this new exclusive endocrinology series on hyperthyroidism describes the steps involved.
Biochemical laboratory assessment
The initial test is usually thyroid stimulating hormone (TSH) test, which if suppressed prompts the full panel of thyroid hormone testing (T4 & T3). TSH has the highest sensitivity and specificity for hyperthyroidism; one can also order the full panel of tests. The serum level of thyroid-stimulating immunoglobulins or TSH receptor antibodies helps distinguish Graves` disease from other causes of hyperthyroidism.
Patients with critical or acute illness often develop the non-thyroidal illness syndrome (also called as sick euthyroid syndrome) manifesting as mildly decreased TSH levels and normal or mildly decreased T4 levels. It resolves spontaneously when the patient recovers from the acute illness. Medications such as exogenous glucocorticoids or dopamine may cause a mild decrease of TSH levels, a situation often occurring in the intensive care unit.
Thyroid isotope scans
After the biochemical tests indicate towards hyper-functioning thyroid gland, the next step is to do a nuclear imaging test – which can be either a technetium scan or a radioactive iodine uptake test depending upon the availability at the treating centre. In case the facilities are unavailable, or the patient does not want to undergo isotope scans, TSH receptor antibody testing may be done, but will identify only Graves` disease rather than other forms of overactive thyroid gland.
These tests determine the uptake of the respective isotopes depending upon which test has been requested. The uptake is very low or negligible in patients with thyroiditis and increased in patients with Graves` disease, a toxic adenoma, or a toxic multinodular goitre. The thyroid scan shows the distribution of radiotracer in the gland. A homogeneous distribution indicates Graves` disease, but accumulation of radioisotope in one area points to a toxic adenoma or in multiple areas to a toxic multinodular goitre.
Ultrasonography is sometimes used as a cost-effective and safe alternative to radioactive iodine uptake and scan. It is the primary imaging modality used during pregnancy, lactation, and in amiodarone induced thyrotoxicosis. Appropriate treatment of hyperthyroidism requires appropriate aetiological diagnosis, along with various patient associated factors like age, pregnancy, and safety profile.
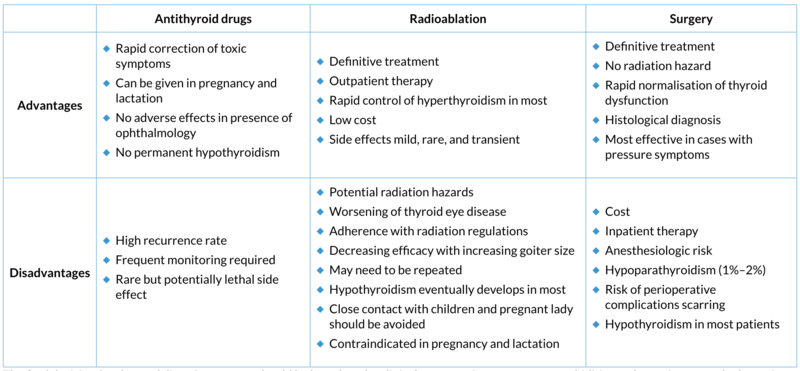
Treatment of hyperthyroidism involves the following modalities:
- Antithyroid drugs
- Radioactive iodine therapy
- Surgery
Antithyroid drugs
The antithyroid drugs available are methimazole, carbimazole, and propylthiouracil (PTU). These drugs act by inhibiting TPO-mediated iodination of TG to form T4 and T3 within the thyroid gland. PTU also blocks peripheral T4 to T3 conversion. Carbimazole is a precursor of methimazole that is rapidly metabolised to methimazole. Additionally, these drugs may have immunosuppressive effects that may be responsible for the remission from the disease that some patients have after 1 to 2 years of treatment.
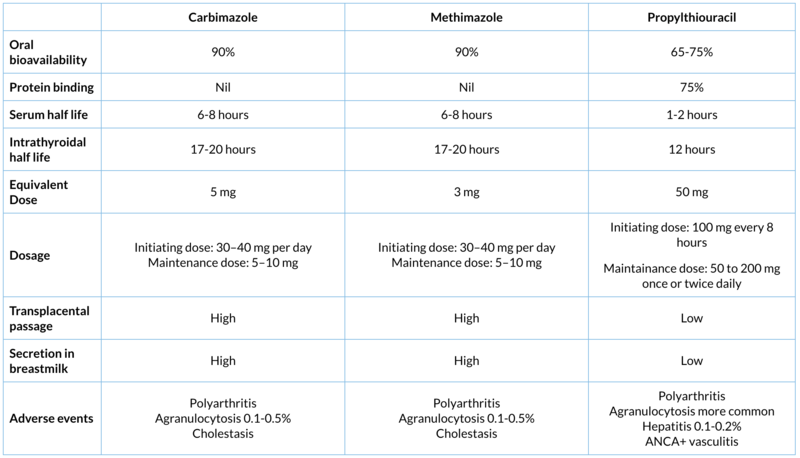
Generally, antithyroid drug therapy is started in full initiating dose and once the patient becomes biochemically euthyroid after 4 to 12 weeks, maintenance therapy is continued with a lower dose for about 18 to 24 months. Due to potential for severe hepatotoxicity with PTU, carbimazole/methimazole is the antithyroid drug of choice, which has fewer side effects, single daily dosing regimen and better compliance. PTU can be considered in patients with mild allergic reactions to methimazole who prefer to remain on antithyroid drugs and is preferred in pregnant women in the first trimester because of better foetal safety.Antithyroid drug therapy as first-line therapy is most useful in young patients with small glands and mild disease. The drug is given for 1 to 2 years, and then it is tapered or discontinued. Remissions, defined as normal thyroid function for 1 year following discontinuation of the antithyroid drug, occur in 20 to 50% of patients, which may not be lifelong.
Radioactive iodine therapy
Introduced in the mid-1940s, radioactive iodine therapy has become the most widely used for hyperthyroidism. RAI is considered effective, safe, and relatively inexpensive. The isotope of choice is 131I. It is given orally and is absorbed rapidly and completely, after which it is concentrated, oxidised, and organified by follicular thyroid cells. The ionising effect of β particles, destroys the thyroid cells by an early inflammatory response, necrosis of follicular cells, and vascular occlusion. Consequently, inflammation and fibrosis result in a decrease in thyroid size and inability to secrete thyroid hormone.
131I is the preferred treatment for most patients of hyperthyroidism over age 21. It is the treatment of choice in patients with toxic adenoma. It is also preferred in patients with Graves’ disease who are elderly and have large goitre (grade III) or comorbidities like cardiac failure or past history of thyrotoxic periodic paralysis. In many patients without underlying heart disease, radioactive iodine may be given immediately in a dosage of 80 to 200 μCi/g of thyroid weight estimated on the basis of physical examination.
Following the administration of radioactive iodine, the gland will shrink, and the patient will usually become euthyroid over a period of 2 to 6 months. In elderly patients and in those with underlying heart disease or other medical problems, severe thyrotoxicosis, or large glands (>100 g), it is advised to achieve a euthyroid state prior to 131I therapy, because there may be exacerbations of thyroid function in the weeks following radioiodine therapy. Patients usually are treated with methimazole until they are euthyroid, medication is then stopped for 3 to 7 days, and the radioiodine therapy is given.
Not all patients respond to 131I and these patients may require multiple doses at 6 to 12 monthly intervals. Factors for poor response are:
- Age (>40 years)
- Female sex
- Severe hyperthyroidism
- Medium or large goitres (>40 g, visible)
- ATD pre-treatment (especially with propylthiouracil)
Hypothyroidism is the almost inevitable complication of radioactive iodine therapy, developing in more than 80% of patients who are adequately treated. Hypothyroidism usually occurs in the first 6 to 12 months after therapy and is the best assurance that the patient will not have a recurrence of hyperthyroidism.
Serum FT4 and TSH levels should be followed up every 6 to 8 weeks, and when hypothyroidism develops, prompt replacement therapy with T4, 0.05 to 0.2 mg daily, is started. Severe Graves eye disease is a contraindication to radioiodine therapy; radioiodine can exacerbate eye problems when they are present at baseline and can even induce mild eye disease in those without eye disease.
Patients with severe underlying hyperthyroidism, very high TSAb titres, and who smoke cigarettes are particularly prone to an exacerbation following radioiodine treatment. It can be prevented by the administration of prednisone 0.4 mg/kg/d for 1 to 2 months following radioiodine therapy. Pregnancy and lactation are absolute contraindication for the use of Radioiodine therapy and urine pregnancy test is mandatory prior to radio-ablative therapy.
Surgery
Although the oldest and most definitive treatment for Graves’ disease is surgery, it is now the least preferred treatment. The procedure of choice is near total thyroidectomy or total thyroidectomy. There are few indications for surgery in Graves’ disease:
- Patient preference
- Large goitres which are causing compressive symptoms or cosmetic reasons
- Graves’ disease super imposed on endemic goitre with multiple cold nodules
- Suspicion of malignancy
- Associated with ophthalmopathy
Surgery should be set only when a normal metabolic state has been restored as thyroid storm might be precipitated in hyperthyroid state. This is done with ATD and Beta blockers. Once eumetabolism is achieved, saturated solution of potassium iodide or Lugols solution is added, 2 to 3 drops twice or thrice daily, for 7 to 10 days before surgery.
The final decision for the modality of treatment should be based on the clinical presentation, age, sex, comorbidities and most importantly the patient preference.
This is second in the series on hyperthyroidism. Click on the following links to read the previous article in the series.
ABC of Hyperthyroidism: What complications should physicians be aware of?- Dr. SK Wangnoo
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The authors of this article are Dr. Subhash Kumar Wangnoo and Dr. Khwajamuhammad Usman KY.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
