Global Longitudinal Strain (GLS) Vs. LVEF: A Complementary Comparison in Echocardiography
M3 India Newsdesk Sep 08, 2023
This article emphasises GLS as a vital substitute or addition to LVEF in cardiac assessment, particularly for early dysfunction detection and condition diagnosis. It includes a practical case and a multiple-choice question to illustrate GLS's clinical importance.
Left ventricular ejection fraction (LVEF) is the established method for the evaluation of LV systolic function and can be measured by a number of imaging modalities. LVEF by echocardiography has been regarded as a cornerstone in the prediction of outcomes and is the most widely available method for the evaluation of LV function.
It is a vital measurement when determining whether patients benefit from an implantable cardioverter-defibrillator (ICD) or cardiac resynchronisation therapy (CRT). In addition, LVEF is used to define systolic heart failure and has a great impact on the selection of medical treatment (HFPEF VS HFrEF).
Limitations of LVEF for LV function assessment
- Reproducibility: inter and intra-observer variability.
- Different methods: 2D ECHO vs 3D ECHO vs MRI; Different result.
- Preload and afterload causing alterations.
- Limitations caused by LBBB or post-surgery abnormal septal motion.
- In an accurate assessment by eyeballing at the very high or low ventricular rate and in the presence of frequent ectopics.
- RVEF by 2D is very inaccurate, so is there any better guidance with GLS?
Use of GLS
1. Use of GLS by speckle tracking imaging helps to identify preclinical LV dysfunction in patients with cancers on potential cardio-toxic chemotherapeutic drugs like anthracycline and trastuzumab even before LVEF drops.
Expert Consensus definition of Cardiac toxicity:
- Drop in EF by >10% to a value of <53%
- Repeat in 2 -3 weeks
- Could predict Cardiac Toxicity: Drop in GLS >15% or 3% absolute value

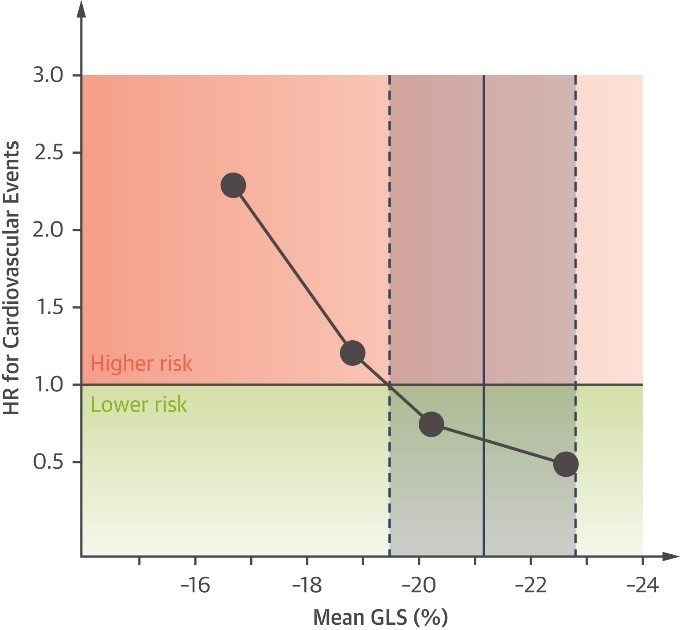
2. GLS is superior to LVEF in predicting poor prognosis in patients with HFrEF.
3. GLS has lesser inter-observer and intra-observer variability and is more reproducible.
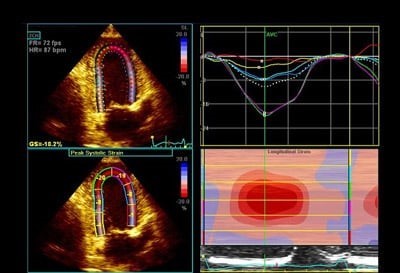
4. Parameters of longitudinal strain for each myocardial segment can be plotted on the bull’s eye and colour rendered, this can help quick evaluation and diagnosis.

Figure: Bull’s-eye plots of peak systolic strains (top panels) and segmental longitudinal strain curves (bottom panels) of the apical (A) 2- and (B, C) 4-chamber views. (A) Infarcted segments show reduced strain and post-systolic shortening (light blue, yellow). (B) Hypertrophic segments deform less (mid and basal segments). The apex might appear spared. (C) Amyloidosis shows frequently an apical sparing pattern. Colour labels of the segments in the bull’s-eye plots correspond to the strain curves. AVC = aortic valve closure; MVC = mitral valve closure
5. Strain measured by speckle tracking is superior as it is angle independent needs a lower frame rate and takes less time to process as compared to tissue Doppler imaging.
6. The predominance of longitudinal fibres in a subendocardial layer which was earliest subjected to ischaemia explains why longitudinal followed by circumferential and in the last radial strain is affected by ischaemia.
7. Athlete heart vs. HCM.
8. RV Strain: Mainly longitudinal fibres
- Easy to perform
- Has diagnostic and prognostic features
9) In Severe AS EF remains normal for long times as increased wall caused by wall thickening is compensated by reduction cavity size. GLS is significantly reduced in early stages and increased circumferential strain (which contributes more to EF) compensates to preserve EF. GLS is being explored as a marker for surgery (AVR) timings before the heart decompensate for better results.
Case illustrations
A) A 77-year-old man, a doctor by profession presented with a history of acute shortness of breath with sweating and anxiety. His EKG revealed STEMI with STE in V1-V6, I,avL suggestive of extensive anterior wall MI. His echocardiogram revealed severe LV dysfunction with EF of 28% and RWMA with severe hypokinesia of mid and apical IVS and lateral wall, anterior wall with akinetic apex.
However, speckle tracking imaging revealed an evil eye pattern on a bull plot which led to suspicion of Takotsubo CMP.

Left polar map of peak systolic longitudinal strain obtained from a Takotsubo syndrome (Our patient) and right polar map of typical anterior ST-segment elevation myocardial infarction patient (for comparison to our patient).
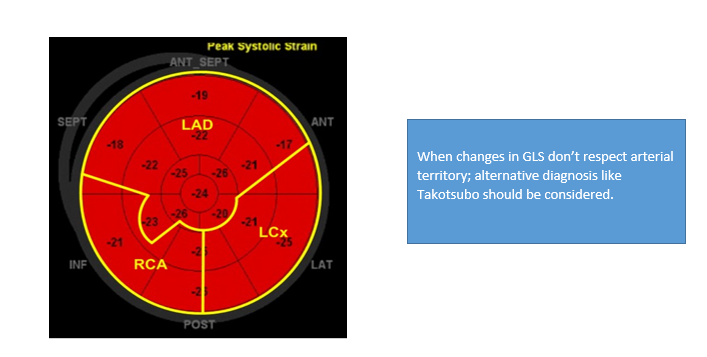
His CAG was done which revealed non-critical CAD.His Troponin and CPKMB were raised. He was diagnosed and managed as a case of Takotsubo CMP.
B) A 71-year-old man presented with progressive and profound fatigue, weight loss and palpitation. His past medical history was notable for bilateral carpal tunnel syndrome 10 years earlier. Electrocardiogram showed low voltage in the limb leads, poor R wave progression and atrial fibrillation. The echocardiogram showed a severely increased wall thickness.
Although ejection fraction (EF) was preserved, longitudinal function by tissue Doppler was markedly reduced. As shown in the image below, the longitudinal strain demonstrated a distinctive apical sparing pattern.
The sum of apical segmental strain values was greater than the sum of mid and basal segmental strain values in the “bull’s eye” strain plot (image below), a finding that has been shown to be sensitive and specific for cardiac amyloidosis.
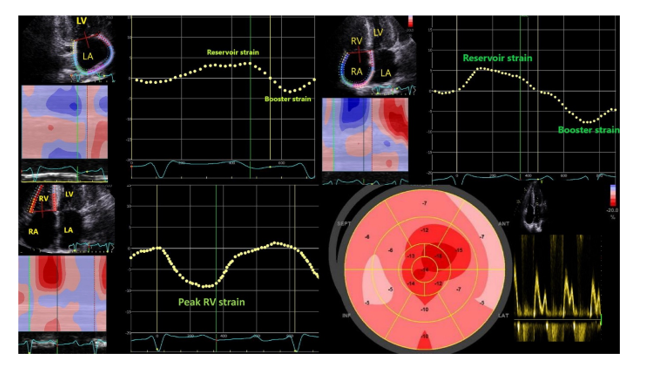
Figure: Bulls plot showing classical cherry on top pattern with speckle tracking imaging on RV
The patient will need a technetium pyrophosphate cardiac scan with SPECT CT, which will confirm the diagnosis. Genetic testing will be done after confirming to point out specific mutations.
Test your knowledge!
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
