Earwax Removal: Best Practice Techniques for Physicians
M3 India Newsdesk Jul 13, 2023
The ceruminous gland secretions and desquamated skin combine to form the ear wax, which traps foreign objects and lubricates the ear canal. This article addresses a variety of wax removal techniques, including syringing, softening chemicals, and microscopic/endoscopic suction toilets.
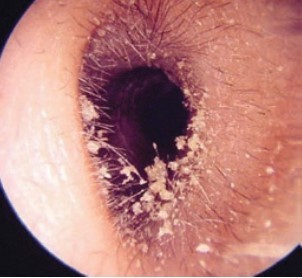
Ear wax is produced by the hair-bearing skin of the external auditory canal. It is a combination of desquamated skin and cerumen formed by glands in the base of the hair follicles. The external canal's outer third contains hairs.
Most external canals are self-cleaning with the desquamated skin migrating up to the hair follicles where it is separated from the dermis and mixes with the cerumen to form wax. The wax leaves the ear canal by moving down the hair. The most common finding is partial occlusion of the canal. In the majority of patients, this will be an incidental, symptomless finding. (1)
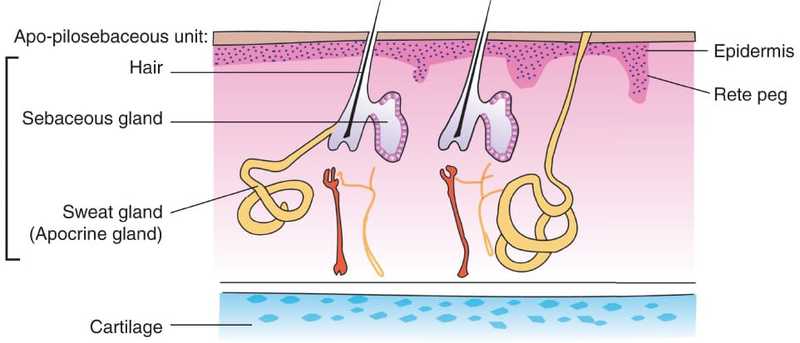
Sebaceous and ceruminous (modified sweat glands) glands open into the space of the hair follicle. Both of these glands' secretions combine with keratin and desquamated epithelial cells to create wax. This lubricates the ear canal and entraps the foreign material that enters the canal.
Usually, a small amount of wax is formed which dries up and is expelled from the meatus by movements of the jaw. (2)
 (1)
(1)
 (2)
(2)
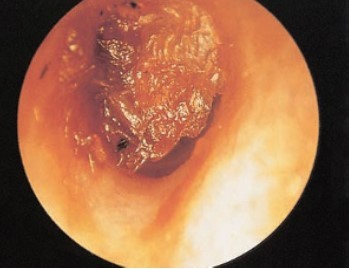
In those with otological symptoms, the wax will need to be removed to enable the canal and tympanic membrane to be assessed. Excessive wax secreted by the glands is deposited as a plug in the outer EAC. It is relatively infrequent for wax to cause a hearing impairment. It requires the wax to be impacted deep in the canal by the use of cotton buds or an ear mould for it to act like ‘ear defenders’ that are used to limit noise exposure. (1)
Wax is often removed by non-specialists by water syringing most commonly using a pressure-controlled irrigator. Specialists ( E.N.T) prefer to remove wax under direct vision with the aid of a headlight, microscope or endoscope, often via a speculum with ear wax hooks, Jobson Horne probes or suction irrigation.
Components of ear wax
The ear wax is made up of the following components:
- Sebaceous gland’s secretion, which is rich in fatty acids
- Ceruminous gland’s secretion, which is rich in lipids and pigment granules
- Hairs
- Keratin and desquamated epithelial detritus shed from the TM and bony meatus
- Dirt (2)
Factors facilitating ear wax problem
The following are the factors, which facilitate the wax problem:
- Wax retention is made easier by the ear canal's narrow and tortuous shape, stiff hair, and exostosis. Wax can then dry up and harden into an impacted mass.
- Excessive secretion of wax and dusty occupations result in an increased amount of wax.
- Self-cleaning of ear wax may push the wax into the deeper bony EAC.
Clinical features of patients with impacted wax
- Hearing loss or sense of blocked ear: Sudden hearing loss may occur when water enters into the EAC (wax swells up) while bathing or swimming.
- Tinnitus and giddiness due to the impaction of wax against the TM.
- Reflex cough can result from the stimulation of the auricular branch of the vagus nerve.
- Wax granuloma: The impacted wax causes ulceration of the meatal skin and the development of granulomas.
Treatment
It consists of the removal of wax by either syringing or other ear instruments.
1. Wax softening agents
Typically, a hard impacted mass needs to be softened beforehand using one of the following wax softening treatments.
- Five per cent soda bicarb in equal parts of glycerin and water
- Hydrogen peroxide
- Liquid paraffin
- Olive oil
- Paradichlorobenzene 2%
Removal
- Always use experienced hands to manipulate instruments, preferably while using ear microscopy. In general, a cerumen hook, scoop, or Jobson-Horne probe is utilised.
- Wax hook and Vectis are used for removing wax, foreign bodies and debris from the external ear canal. In cases of impacted wax, a space is created between the wax and the canal wall.
- The wax lump is then pulled out once the instrument has been passed past it. If the lump breaks, syringing or suctioning may be used to remove the fragment. (2)
2. Ear toilet
In primary care, the ear toilet is mainly confined to the clearance of wax. Clearing up tough places, such as the attic and open mastoid cavities, is substantially aided by doing toilet under direct eyesight, especially if this is enlarged with a microscope or endoscope.
Patients will tolerate extensive toilets better if they are in a relaxed position on a reclining chair or couch. They should be informed as to what to expect, especially the noise of suction or irrigation of water. The latter on occasion can cause a short episode of vertigo especially if the irrigation fluid is not at body temperature. (1)
3. Syringing
Syringing to remove visually obstructing wax or wax considered potentially to be causing a mild hearing impairment is now most frequently performed by suitably trained, paramedical staff.
As this is most often not performed under direct vision and the otoscopic diagnostic skills of the operator will be limited, there are usually firm contraindications to syringing. So ears with a discharge or previous ear surgery do not ideally undergo this procedure. (1)
4. Microscopic/endoscopic suction toilet
Ear toilet with magnification is popular among specialists as it allows the external canal and tympanic membrane to be magnified while wax, pus or debris is removed using a suction cannula or other instrument. The magnification afforded by the microscope or endoscope allows the ear to be cleaned with great precision and with minimal patient discomfort. Irrigation of troublesome areas with a small syringe filled with water often aids the process. Because this toilet is used in plain sight, harmful consequences like injury to the ear canal, tympanic membrane, or middle ear are rare. Haemorrhage, if it occurs, can be easily controlled. (1)
Method
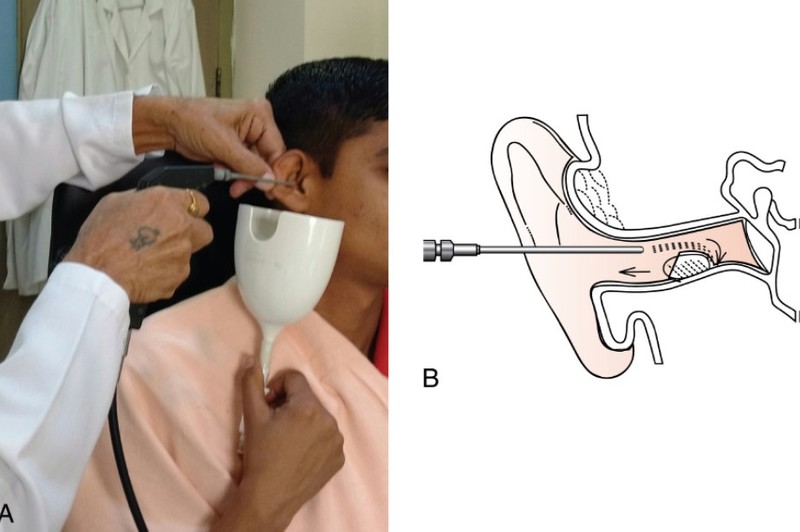
The patient is seated comfortably and the diseased ear faces towards the doctor. A towel is placed on the shoulder. The patient’s head is slightly tilted toward the shoulder. The return fluid is gathered in a kidney tray that is tightly held deep below the ear. It uses boiled tap water that has been cooled to body temperature (or regular saline).
The auricle is pulled upwards and backwards while the direction of the stream of the ear syringe is towards the posterosuperior wall of the meatus. The pressure of water that builds up deeper into the wax expels the wax out. When the wax is hit, a gap is made between the wax and the meatal wall, allowing a stream of water to pass through.
Otherwise, the wax would be pushed deeper. After the procedure, the ear canal and tympanic membrane are dried with cotton.
Cautions
- A ruptured TM from excessive syringing force can cause excruciating pain, lightheadedness, and fainting.
- Before beginning the syringing, it is important to inquire about previous ear discharge or an existing perforation. After syringing, a dormant otitis media may become active again.
- Too cold or too hot water would stimulate the labyrinth and result in vertigo.
- Ulceration in meatal wall needs the application of broadspectrum antibiotic ointment. (2)
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Tosha Shah MS is a Senior Consultant practitioner at Dhiraj Hospital, Vadodara.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
