Ear Infection in Paediatric Patients
M3 India Newsdesk May 19, 2023
Children are more vulnerable & prone to upper respiratory tract infections than other age groups, specifically focusing on three common conditions. The causes, stages, & treatments of each condition are explained, along with case scenarios to illustrate their presentation & management.
Paediatric ear infections
The paediatric age group is particularly more vulnerable and susceptible to upper respiratory tract infections. Through interconnections of lymphatics in Waldeyer’s ring an enlarged adenoid or recurrent tonsillitis can lead to several middle ear infections such as acute otitis media or serous otitis media brought upon by eustachian tube dysfunction.
The chronicity of the condition can lead to chronic otitis media. Adding to this serious consequence is the immaturity of bone development of the mastoid leading to disastrous end results.
With the advent of antimicrobials, the results are almost manageable with almost nil mortality and a rapidly declining morbidity.
The three most common diseases in the paediatric age group
Acute otitis media is defined as an infection of the middle ear space. It is a spectrum of diseases that includes acute suppurative otitis media (ASOM), otitis media with effusion (OME) and chronic suppurative otitis media (CSOM),. Acute otitis media is the second most common paediatric diagnosis in the emergency department, following upper respiratory infections. Although otitis media can occur at any age, it is most commonly seen between the ages of 6 to 24 months.
1. Acute suppurative otitis media (ASOM)
It implies an acute pyogenic inflammation of the middle ear cleft, which includes ET, middle ear, attic, aditus, antrum and mastoid air cells. Though AOM can occur in all ages, it is mainly the disease of children as the ET is shorter, wider and more horizontal and opens at the lower level in children. Both ears may be involved. (1)
Any pathology that interferes with the normal functioning of the eustachian tube predisposes to a middle ear infection. It could be:
- Recurrent attacks of common cold, upper respiratory tract infections and exanthematous fevers like measles, diphtheria or whooping cough
- Infections of tonsils and adenoids
- Chronic rhinitis and sinusitis
- Nasal allergy
- Tumours of the nasopharynx, packing of nose or nasopharynx for epistaxis
- Cleft palate
Typically there are 5 stages of AOM:
- Stage of tubal occlusion
- Stage of pre-suppuration
- Stage of suppuration
- Stage of resolution
- Stage of complication (1)
The treatment protocol used is :
It remains the same for adults and paediatric age groups:

Case scenario: Generally, the patient is present in the first or second stage itself, thereby decreasing the number of complications associated with ASOM. Patients have a nidus of infection in the throat i.e. recurrent tonsillitis or acute exacerbation of it or adenoid hypertrophy. The subclinically treated patients may develop OME or progress to CSOM.
2. Otitis media with effusion (OME)
It is the accumulation of mucus within the middle ear and sometimes the mastoid air cell system. Persistence of the fluid for the condition to be described as chronic is normally taken as 3 months or longer. In children, OME may present with hearing loss but also delayed speech and language development, poor social behaviour and, in younger children, difficulties with balance.
As a rule of thumb, we must always rule out the presence of hypertrophied adenoids occupying and occluding the nasopharynx. Hampering the physiological functioning of the eustachian tube.
The ventilation of the middle ear, along with the draining of liquids into the nasopharynx via the continuous beating of cilia, stops. This leads to fluid collection in the mesotympanum, leading to aural fullness and the above-mentioned symptoms. (2)
Case scenario: A 9-year-old Muslim male child attended our OPD with complaints of aural heaviness with ear itching. The patient had complaints of mouth breathing with snoring at night. The patient had a post-nasal drip on examination indicating adenoid infection. The tympanic membrane was bulging on both sides and the xray soft tissue lateral view of the skull showed significant adenoid hypertrophy obstructing the posterior choana of the nose. The patient showed moderate conductive hearing loss with a type B curve on impedance audiometry, indicating fluid behind the tympanic membrane hampering the conduction of sound. The patient underwent tonsil adenoid resection along with bilateral ear grommet insertion in the anteroinferior quadrant of the tympanic membrane. (3)
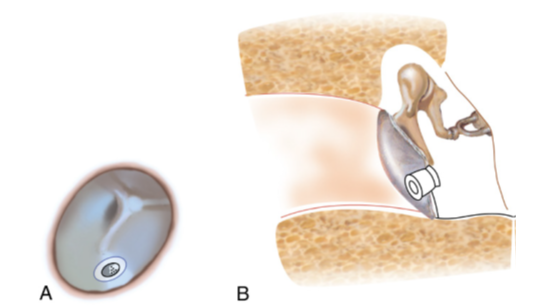
Grommet in the tympanic membrane (A and B). (3)
3. Chronic suppurative otitis media (CSOM)
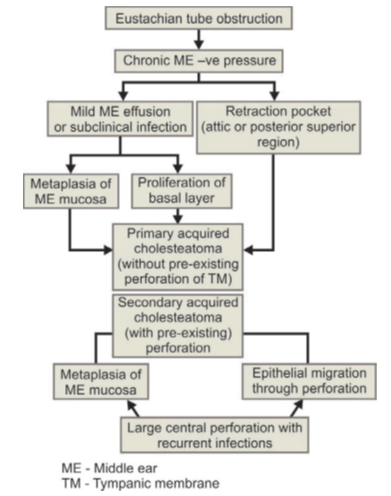
It is a long-standing infection of the middle ear cleft. It is characterised by ear discharge and a permanent perforation of the tympanic membrane. The perforation edges are covered by squamous epithelium. It does not heal spontaneously and becomes a sort of epithelium-lined fistulous track. Two types are as follows:
Tubotympanic type (safe or benign): This type of CSOM involves the anteroinferior part of the middle ear cleft and is associated with a permanent central perforation. As there is no risk of serious complications, it is called safe or benign CSOM.
Atticoantral type (unsafe, dangerous, posterosuperior lesion or cholesteatoma): This type of CSOM involves the attic and posterosuperior regions of the middle ear cleft. It is associated with an attic or marginal perforation in the posterosuperior quadrant of the pars tensa. As it is often associated with a risk of serious complications because of the bone erosion nature of cholesteatoma, it is called unsafe or dangerous CSOM. Granulations and osteitis are present in many cases. (1)
The majority of the children presenting to us in our centre have distinct foul-smelling ear discharge, and yellowish discharge many presenting late with manageable complications. Mastoid surgery is necessary in all these cases, especially in young ones with unsafe ears. Mastoid surgery gives the patient 5 D’s, i.e. dizziness, deafness, discharging cavity, doctor dependence and defect. All these are manageable as opposed to the risk that the disease carries of infecting and invading brain parenchyma. Modified radical mastoidectomy is carried out to remove all the unhealthy, infected tissue. Augmentation surgery and hearing mechanism id reconstructed in the same setting in our centre. Any paediatric patient with foul-smelling ear discharge is treated with urgency and treated promptly because the spread of disease is fast as mastoid bone is still developing: providing fragile bone and blood vessels aiding in the sped-up process of progression of disease along with complications.
If the perforation is encountered in the safe ear; the causative factor is first treated and generally patient is asked to wait till adulthood for tympanoplasty as many children undergo remission unprompted. But symptom control is of utmost importance. Also, hearing shouldn’t suffer as it would result in speech difficulties. Understanding -the above-mentioned topics appropriate decision is made.
Aetiology
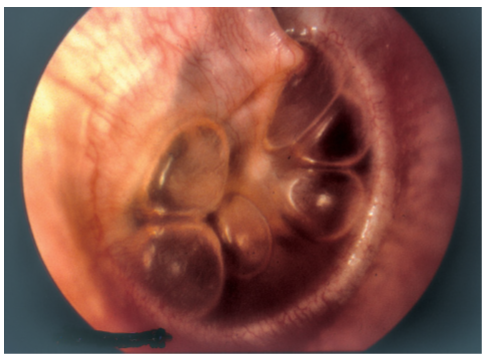
Case photos:


Ear: Microscopic picture showing grade 4 attic retraction with the complete lateral wall of attic destruction signifying an unsafe ear.
In this article, I have only brushed upon the utmost necessary topics. There are many more, but the above ones are the most frequently encountered in our OPDs.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Tosha Shah MS is a Senior Consultant practitioner at Dhiraj Hospital, Vadodara.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
