Anaesthetic Management in Obese Patients
M3 India Newsdesk Nov 07, 2024
This article provides a comprehensive overview of managing obese patients undergoing surgery, using a case study of a 23-year-old female with acute cholecystitis posted for laparoscopic cholecystectomy.
Obesity is defined as a body weight that exceeds the expected body weight or ideal weight by more than 10%, considering height, age, body build and sex.
In adults, the World Health Organisation and the National Institute of Health define obesity as a BMI greater than or equal to 30kg/m². Morbid obesity is defined as actual weight exceeding twice the ideal body weight (IBW).
It is essential to know the anatomy and physiologic changes in obesity, and drug dosing is very important in these patients compared to patients with normal BMI.
Below is the case management of an obese patient diagnosed with acute cholecystitis with cholelithiasis posted for elective surgery for laparoscopic cholecystectomy.
Case report
A 23-year-old female came with complaints of right abdominal pain for the past 2 days with 2-3 episodes of vomiting. She was recently diagnosed with Type 2 Diabetes mellitus which was under control with insulin treatment (Inj Human Mixtard 30/70 20U - X - 20U)
On clinical examination, right upper quadrant tenderness was present, Height 165cm, Weight - 96 kg, BMI 37.5 kg/m² and PR - 96 bpm, BP - 130/70 mm/hg, Auscultation was normal, and the chest was clear.
Airway examination was normal ( MPG 2, TMJ > 6.5cm, mouth opening was adequate) Spine examination was normal.
Investigations
-
Hb 11.5 g/dl, Blood group O+ve, Platelet 2.4 lakhs, LFTs and RFTs were normal. Viral serology for HIV, HBsAg, HCV negative, TSH - 2.02, ECG - Sinus rhythm. Chest X-ray- normal, Coagulation profile PT 14 seconds, INR 1.2 Ultrasound - Multiple calculi were present highest measuring 7mm.
-
She had a history of tonsillectomy done under general anaesthesia at childhood which was uneventful. She was given Inj TT 0.5ml im, Inj ondansetron 8mg iv, and Inj pantaprazole 40mg iv before shifting to the operating room. She was shifted into the operating room and connected with ASA standard monitors.
-
An 18 G IV cannula was secured in the left hand and preloaded with RL 500ml. RAMP position was kept. Difficult airway trolley was kept ready. The patient was premedicated with Inj glycopyrrolate.
-
0.2 mg iv; Inj Fentanyl 100mcg iv; Induced with Inj Propofol 150 mg; Intubated with Inj succinylcholine 100mg; 7.5mm octet and fixed at 22 cm mark after checking bilateral air entry.
-
Intraoperatively warmer was kept. Inj PARACETAMOL 1g iv + Inj Magnesium 2g + Inj demamethasone 4mg iv was given.
-
The patient’s vitals were PR:82bpm, BP 120mm/Hg, SpO2 98% IRA. Initially patient’s BP reading increased to 140/90 mm/Hg after the introduction of trochar and insufflation of CO2 and gradually decreased after maintaining Sevoflurane 1-2% and maintained with O2:Air 1:1. Inj vecuronium 1mg iv was given every 20 mins. Ventilator settings TV -400ml, RR 12bpm, PEEP - 5 cmH2O.
-
Pressure points were padded. The intraoperative period was uneventful. Surgical time was 1 hour 10 mins. The patient was extubated under awake after spontaneous attempts achieved using Inj Myopyrollate 4mg and shifted to the ward. The fluid input was 1100 mL.
-
Postoperatively oxygen support was given with Hudson’s mask 4L min initially and tapered off. Analgesic support with Inj paracetamol 1g TDS was given.
Discussion
- RS - Decreased time to desaturation to apnea and increased oxygen requirements and hypoventilation during supine ventilation.
- CVS - Increased circulating blood volume, decreased systemic vascular resistance, increased cardiac output by 20-30 mL per kilogram of excess body fat, left ventricular hypertrophy related to duration of obesity.
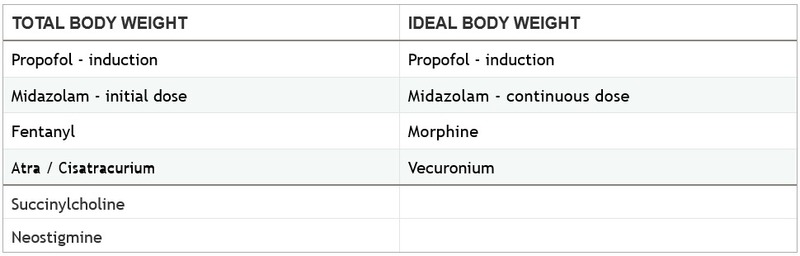
- Drug dosing - An idea of Ideal body weight and Total body weight should be well-understood.
- Associated conditions - Conditions such as Obstructive sleep apnea, Coronary artery disease, Systemic hypertension, Diabetes mellitus, Metabolic Syndrome, and Hypothyroidism should also be evaluated.
- Choice of anaesthetic technique - Regional anaesthesia (Spinal or epidural) without opioids minimally affects the respiratory drive and are safe and appropriate choice for obesity. Also, peripheral nerve blocks with ultrasound seem to be safe.
Anaesthetic challenges in obesity
- Preanaesthetic period - Preoperative use of stockings or low dose subcutaneous unfractionated heparin or low molecular weight heparin can be given to prevent postoperative development of thromboembolism.
- Specific equipment needs - Large or high-weight capacity beds and operating tables are needed. Extra long needles for spinal, epidural and nerve blocks may be needed.
- Appropriate-sized BP cuffs are always required due to their large-sized arms.
- Positioning -. Due to excess pad of fat in the neck, positioning becomes difficult and sometimes RAMP(Rapid airway management protocol) is needed where the patient’s external auditory meatus and sternum come to line in a straight line. The use of a short handle with a blade also seems to be helpful. Pressure-dependent areas are adequately padded to prevent nerve injuries.
- Preoxygenation - Due to reduced FRC(functional residual capacity), morbidly obese patients may desaturate more quickly. It can be prevented by preoxygenation patients in an upright position of 25 degrees and administering oxygen using a 10 Fr catheter through the nasopharynx at 5L/ min.
- Airway management - Difficult mask ventilation and intubation may be more challenging. If anticipated difficult intubation is present, prefer awake intubation. Difficult airway trolley including flexible fibre optic bronchoscopy, adequate size masks and blades, airways and supraglottic airway devices, bougie should be kept ready.
- Intraoperative drugs - Some drugs should be given according to Total Body weight and Ideal Body weight.
Extubation - The trunk and head up position during extubation improves oxygenation and the work of breathing. Avoid premature extubation especially in obese patients as re-intubation is difficult in cases of airway oedema.
Post-operative oxygen support- Obese patients are prone to desaturation, especially in the postoperative period and providing oxygen support either with Hudson’s mask or with non-invasive ventilation such as CPAP(continuous positive airway pressure) helps to prevent respiratory complications such as pneumonia or lung collapse.
Multimodal analgesia - Multimodal opioid-sparing analgesic strategies including nonopioid analgesics ( paracetamol), NSAIDS, local wound infiltration, and peripheral nerve blocks alleviate the pain in the postoperative period.
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Vignesh N, MD (Anaesthesia & Critical Care) is an Assistant Professor at Meenakshi Medical College and Research Institute in Kanchipuram.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
