"Abdominal pain: Order tests only after considering provisional diagnosis"- Dr. YK Amdekar
M3 India Newsdesk Jun 12, 2019
Dr. YK Amdekar, in his new CME and Quiz series, explains the diagnosis and evaluation, identification of red flags, and the steps to be taken when a patient complains of abdominal pain, but the physical examination is normal.

Before you begin, take the quiz below to test your knowledge.
What is pain?
Pain is unpleasant sensory and emotional experience arising out of an underlying cause. It helps an individual to guard against it. Pain stimulates pain receptors that are present in all organs (except brain, lung parenchyma). It is transmitted via nerves to spinal cord and then to brain where it is processed. The brain thereafter sends message down the spinal cord via specific nerves to initiate desired action. It is also important to note that pain can arise from diseases of nerves as well and such a pain is burning or like an electric shock.
Anatomy and physiology related to abdominal pain
Abdominal contents are divided into foregut, midgut and hindgut. Foregut represents pharynx, oesophagus, stomach, liver, gall bladder, pancreas while midgut represents duodenum, caecum, and appendix while hindgut represents colon, rectum and part of anal canal. Each section has visceral afferent nerve that transmits pain to spinal cord via autonomic sympathetic nerve. Visceral afferent nerve thus represents non-specific area.
There is an overlap between visceral nerve and somatic nerve that is specific to a particular area. That is how pain from visceral organ is first felt at the distribution of somatic afferent and hence pain from inflamed appendix is first felt at periumbilical region – T10 level and then shifts to right iliac fossa at T12 level where appendix is situated.
Specific quadrant pain is related to the organ situated in that quadrant. However some quadrants contain more than one organ. At times, pain in right hypochondrium may represent lower lobe pneumonia and may be mistaken for pain arising from liver. Similarly, as kidney lies in posterior compartment, pain manifests at renal angle on the back.
Types of abdominal pain
Visceral pain arises from abdominal organs as a result of stretch, inflammation or ischemia. It is dull, poorly localised superficial, often referred to distant area from the site of involved organ. It is accompanied with autonomic symptoms such as nausea, vomiting, sweating and feeling sick. As against parietal pain represents involvement of peritoneum, it is sharp, severe and well localised to the site of involved organ.
This is how as mentioned above, appendicular pain starts in midline and gets localised to right iliac fossa with increasing severity once the peritoneum is affected. If hollow organ is involved, pain is colicky with intermittent pain-free period and if solid organ is involved, pain is dull and continuous.
Pathogenesis of pain
- Most common cause of pain is inflammation. Inflammation is mostly a result of infection but also due to non-infectious causes such as systemic inflammatory diseases and malignancy.
- Vascular pain results from ischaemia and is localised to the part supplied by affected artery.
- Stretch leads to pain as happens if liver capsule is stretched.
- Psychogenic abdominal pain is common in older children and is caused by stress.
- Referred pain may present at the distant site from affected organ as happens in back pain arising from renal disease.
- Neurogenic pain is localised to area supplied by affected nerve and usually seen in affection of peripheral nerves, thus not applied to abdominal pain (rarely herpes zoster may present with severe superficial burning pain in a localised part innervated by a single nerve and diagnosis becomes apparent only after vesicular skin rash appears a day or two later).
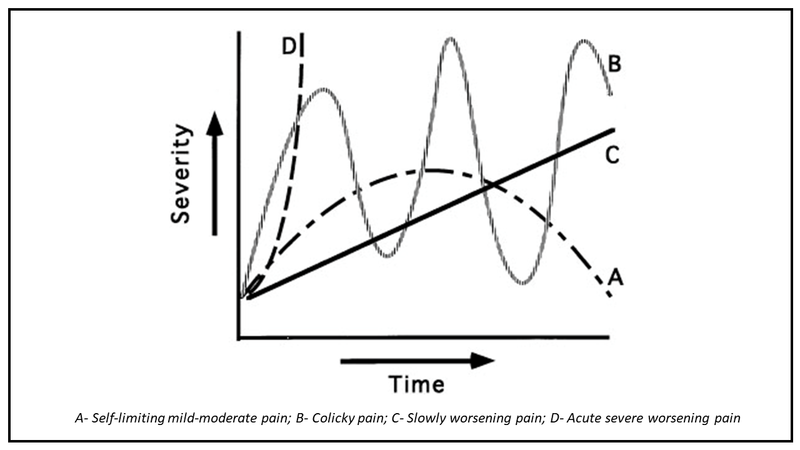
Onset, duration, and progress- a good guide
- Sudden onset of severe pain is often mechanical (renal or biliary calculus, intestinal obstruction, ovarian torsion – mostly surgical) or vascular (include five types of lesions - vasculitis, vasculospasm, thrombosis, embolism and haemorrhage – mostly medical)
- Onset of pain over few days preceded by fever is typically an inflammatory pain and may also have additional symptoms depending on which organ is involved (loose stools with blood and mucus in bacillary dysentery, nausea, vomiting followed by jaundice in viral hepatitis, severe periumbilical pain with vomiting in appendicitis)
- Severity of pain suggests severe inflammation as in case of liver abscess or appendicitis while viral hepatitis often has mild pain
- Recurrent pain with intervening normal period suggests colicky pain coming from hollow tubular structures such as intestines, ureter or bile ducts
- Persistent pain worsening over few hours may indicate surgical cause while persistent pain over days or weeks may be due to gastritis or peptic ulcer (rare in children) and may be psychological, especially if it does not hinder routine activities. It is generally “pain of convenience” – it comes whenever need arises and disappears completely when child is engrossed in what he likes to do
- Worsening pain or one that disturbs health needs cautious evaluation
Physical examination
- Inflammatory pain is accompanied with tenderness besides other localising signs such as guarding or rigidity and such a child is very sick looking.
- Mechanical causes may or may not present with abnormal physical findings. There are no physical findings in renal or biliary colic, so also lead colic.
- Vascular pathology causing pain is devoid of any local tenderness and they include vasculitis, intestinal ischaemia as happens in dengue capillary leak syndrome and shock, sickle cell haemolytic anaemia or Henoch-Scholin purpura.
- In adults diabetes may present with abdominal pain without any local physical abnormality though in children it is rare.
- Abdominal migraine and abdominal epilepsy also present without any physical findings.
Generally the last two conditions are considered when other causes are excluded. Besides local abdominal examination, findings away from abdomen should not be ignored. Degree of sickness, dehydration or electrolyte – acid-base imbalance must be noted in every child. Affection of other systems offers clue to a disease with multiorgan involvement as seen in inflammatory bowel disease with arthritis or sickle cell anaemia with pallor and splenomegaly.
When physical examination is normal!
In presence of abnormal physical findings such as localised tenderness, guarding and rigidity or a palpable lump make diagnosis rather easy. But, the real challenge is when there are no abnormal physical findings. In such situations, one must look at personal history in details. Appetite, sleep, playfulness, energy and activity behaviour besides bowel movements and urination- if all are normal, one is nearly certain about it to be functional pain.
However, if any of the above mentioned symptoms are subtly upset, one needs to be cautious. Based on severity of pain and especially if the pain awakens the child- one must find organic cause. Rare conditions such as Meckel’s diverticulum, lead poisoning, porphyria, abdominal migraine and abdominal epilepsy are some of the conditions where there may be paucity of abdominal findings.
Red flags
- Sudden, acute, severe abdominal pain with abdominal distension and vomiting is usually an emergency and there is a need to find the cause to initiate appropriate action. For example, there may be an urgent need for surgical intervention as in case of intestinal obstruction.
- Bile stained vomit signifies intestinal obstruction till proved otherwise. Blood in vomit, blood passed per rectum or purpuric skin rash needs proper assessment as it often signifies underlying serious illness.
- Unanticipated severe abdominal pain presenting few days after the onset of fever indicates complication as happens typically in dengue fever. When fever in such a case is on the wane, sudden appearance of severe abdominal pain suggests capillary leak syndrome with shock during which intestines are not perfused with adequate blood and so suffer ischemic pain. If neglected for a day, it may endanger life.
- Loss of weight in persistent abdominal pain needs evaluation.
- Finally, if a child wakes up from deep sleep with severe pain, it definitely deserves further investigations even in the absence of abnormal physical findings. Though one may come across a child who wakes up happily only to fake severe abdominal pain. Guarding, rigidity, toxic or sick look and signs of shock or sepsis are obvious serious signs.
Investigations to run
Tests must be ordered only after considering provisional diagnosis. Though unfortunately, tests are carried out because one has no clue to any diagnosis. But in such a case, which tests would you order?
So called 'routine' tests are irrational. CBC and routine stool examination mostly do not add any value to diagnosis. In an inflammatory pain, CBC is bound to be abnormal but one has made out inflammation even without CBC. And CBC in such a case fails to define cause of inflammation. Serum amylase or lipase are markedly increased in acute pancreatitis but moderate increase may also be seen in intestinal ischemia or strangulated hernia.
Similarly, stool examination has little value though presence of occult blood may need cautious interpretation. In fact stool microscopy showing worm infestation may not mean cause of abdominal pain is attributed to it. Abdominal USG is not necessary if liver or spleen in enlarged on physical examination as it adds not much greater value to diagnosis. Same is true with CT or MRI scan. USG showing 'probe tenderness on right iliac fossa' or distended loops of intestine or thickened bladder wall need correlation with clinical profile and recently it is an established trend that all tests come with a rider 'correlate clinically'. Imaging reports often have '?' as prefix! But clinicians are supposed to offer definite opinion and not '?' Thus, prerequisite for ordering tests is provisional bedside diagnosis and test results must be correlated with clinical profile.
In summary, abdominal pain is often a challenging symptom. Acute onset of severe abdominal pain needs cautious attempt at early diagnosis for better outcome. Similarly one must rule out potentially serious diseases. Tests must be ordered with the specific aim of getting more relevant information. 'Routine' tests have no value. Management has to be more specific for rational outcome. Empirical treatment must have a justification and should not be polytherapy hoping one of the drugs may work.
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
