Tophaceous Gout: Management and Advancements in Therapies
M3 India Newsdesk Aug 01, 2023
Tophaceous gout is an advanced stage of gout characterised by the deposition of urate crystals, forming visible tophi in joints and soft tissues. Explore management advancements in tophaceous gout, including novel therapies and diagnostic insights, for enhanced patient care.
Introduction
Gout is one of the oldest joint diseases known to humanity. Gout word is derived from “gutta” meaning drop. It is a clinical syndrome occurring as a result of the deposition of monosodium urate monohydrate crystals from hyperuricemic body fluids.
Definition & overview of tophaceous gout
It is an advanced stage of gout, chronic inflammatory arthritis, because of the deposition of urate crystals in the joint & soft tissue to form visible tophi (large, palpable nodule).
Pathogenesis
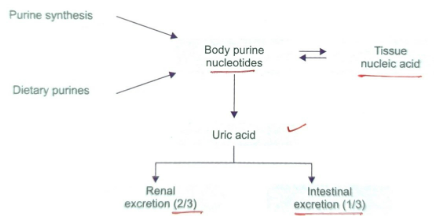
The main culprit of uric acid is purine degeneration production in humans.
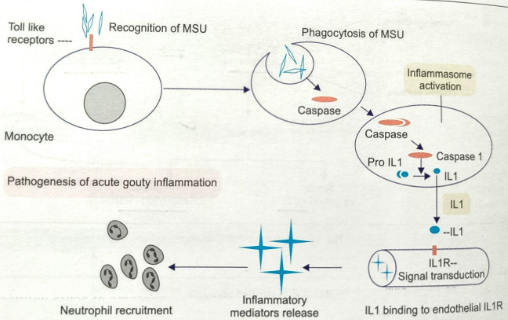
The pathologic hallmark of a gout attack is the neutrophil influx into the synovium and joint fluid, triggered by the interaction between MSU crystals and synovial lining cells.
MSU crystals are phagocytosed by macrophages triggering formations of inflammasomes which result in the formation of proinflammatory cytokines, especially IL 1β. Inflammosomes are multicentric cytoplasmic protein complex which acts as molecular platforms for the activation of inflammatory caspases following stimulation by foreign agonists.
The active form of IL1 binds to the endothelial IL-1 receptor, causing signal transduction, inflammatory mediator release, and neutrophil recruitment.
Clinical presentation
Sporadic acute mono or oligoarthritis to recurrent polyarthritis. Tophi occurs in around 1/3rd of chronic gout patients, often 5-10 years after the 1st episode. The tophi deposit develops around the joints of feet, fingers, elbow, Achilles tendon, and pinna of the ear. Sometimes, this may lead to joint deformity and functional impairment.
Diagnostic approach
Acute or chronic joint pain associated with hyperuricemia is not sufficient. Around 1/3rd of patients have normal serum uric acid levels during the attack (due to the uricosuric action of IL1). So we look for different blood parameters and demonstration of urate crystals and some imaging modalities.
In blood- Raised ESR, raised CRP & neutrophilic leucocytosis.
Demonstration of crystal- Aspiration of joint fluid seen under polarised microscope shows needle-shaped urate crystals, negatively birefringent, (intracellular crystals seen in acute gout and extracellular crystals seen in chronic gout).
Imaging-
- X-ray shows asymmetric inflammatory erosive arthritis, punched out an oval or round defect in the margin with overhanging margin (martels sign) USG- snow storm appearance, double contour sign.
- Conventional CT scan- Can visualise tophi and bony erosion also helpful in scoring bone erosion.
- Dual-energy CT (DECT)- Has the potential to demonstrate MSU crystal depositions, and gives a different colour to materials with different spectral profiles, so it differentiates low-density urate deposits from other denser materials like calcium.
- MRI- Detects joint effusion, synovitis, tendon disorders, tophus, and cartilage disorder or bone oedema.
Differential diagnosis
Chronic tophaceous gout can mimic rheumatoid arthritis with rheumatoid nodules, psoriatic arthritis, or scleroderma, demonstration of urate crystals from tophi and radiological examination of the joint helps in differentiation.
Management
- Medication and lifestyle changes- NSAIDs, colchicine, steroids are used in acute attacks, however, advancements in pharmacologics have expanded the therapeutic arsenals new medications including xanthine oxidase inhibitor (allopurinol, febuxostat) & uricosuric agents (probenecid, lesinurad, benzbromarone, sulfinpyrazone) help lower serum urate level, thus reducing crystal deposition & tophus formation. Lifestyle changes such as dietary modification like decreased intake of purine-rich food, alcohol (beer), red meat, and carbonated drinks, play a critical role in long-term management.
- Biologic therapies- In recent years these drugs emerged as promising options for patients with tophaceous gout who are refractory to conventional treatment or have contraindications. E.g. pegloticase (recombinant uricase enzyme), drugs targeting IL1 –canakinumab, anakinra, rilonacept, IL6 inhibitor tocilizumab. All these have shown efficacy in reducing gout flare & tophi size.
- Surgical intervention- In cases where tophi cause significant joint destruction or deformity, surgery may be needed (arthroscopic or open synovial excision).
Case studies
Case 1. Chronic tophaceous gout with unusually large & multiple tophi
Introduction and clinical presentation
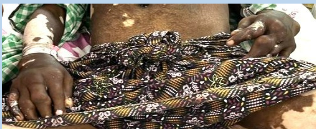
A 40-year-old male presented with nodular growths on b/l feet with generalised pain at b/l knee joint, ankle, and MTP joint. The patient was a known alcoholic. O/E-multiple hard nodular swelling over b/l feet largest being on the right 1st MTP joint of size 5*4 cm, and all nodules with chalky white tip and some with whitish discharge.
Laboratory findings and radiologic examination
Lab reports revealed se uric acid 13.2 mg/dl, ESR-50mm/1st hour, CRP-26mg/L, radiologic examination showed soft tissue swelling & destruction of 1st MTP joint.
Joint fluid analysis
The joint fluid was aspirated and sent for microscopy which showed needle-shaped MSU crystals.
Diagnosis and treatment
The patient was started on allopurinol (100 mg OD) and colchicine (0.5 mg) and the pain was subsided and the uric acid level decreased to 9.2 mg/dl, patient discharged with allopurinol.

(Image 1) Multiple tophi on bilateral foot
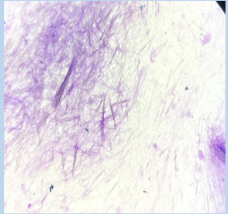
(Image 2) MSU crystals under the microscope
Case 2. Tophaceous gout in a CKD patient
Introduction and clinical presentation
A 60-year-old man with a known case of chronic medical renal disease & vitiligo presented with b/l lower limb swelling and decreased urination and incapacitating pain with nodular swelling over b/l upper limb and lower limbs O/E- multiple hard nodular swelling over foot and hand near the joints with whitish discharge from some nodules.
Laboratory findings
On work up blood reports showed serum uric acid of 19.2 mg/dl and urea, creatinine -102mg/dl, 6.7 mg/dl respectively. ESR- 60/1st hour, CRP-40.
Joint fluid analysis
Synovial fluid aspiration showed needle-shaped MSU crystals.
Radiologic examination
An x-ray of the foot showed joint erosion with martle sign.
Diagnosis and treatment
The patient was started on febuxostat 40 mg and the pain subsided, the patient sends to nephrology.


(Image 3) Tophi over the bilateral foot
(Image 4) Multiple tophi over bilateral hand
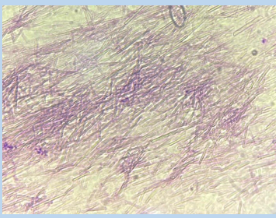
(Image 5) MSU crystals

(Image 6) X-ray showing martels sign and erosions of bone and joint
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Khemeswar Agasti is an MD in General Medicine from Cuttack.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
