KDIGO Guidelines for Management of Blood Pressure in CKD
M3 India Newsdesk Apr 05, 2023
Managing hypertension in chronic kidney disease (CKD) can be quite challenging for primary physicians. Kidney Disease Improving Global Outcomes (KDIGO) has developed guidelines for the management of blood pressure in patients with CKD. This article will summarise the key guidelines' recommendations.
Blood pressure in CKD
CKD patients' blood pressure is not controlled even after combination therapy of three or more drugs. The major risk associated with uncontrolled blood pressure is further deterioration of kidney function along with an increase in the risk of cardiovascular events which overall increases the mortality in chronic kidney disease (CKD) patients.
Lifestyle modification along with proper use of drugs as per guidelines can help physicians achieve blood pressure targets in CKD patients.
This article highlights the important recommendations suggested by Kidney disease Improving Global Outcomes (KDIGO) for managing blood pressure in CKD.
Classification of CKD
Physicians must classify kidney disease patients according to the eGFR. The classification helps the primary care physician to modify treatment as per guidelines structured for different stages and also guides the physician for timely referral to the specialist. Early intervention with lifestyle modification and medicines can delay the progression of chronic kidney disease.

The numbers in the coloured boxes are a guide to the frequency of monitoring (number of times per year)
Blood pressure measurement
- As per recommendation, standardised office BP measurement is preferred to routine office BP measurement for the management of high BP in adults. An oscillometric BP device may be preferable to a manual BP device; the emphasis is on adequate preparation for BP measurement.
- As per recommendation, out-of-office BP measurements with ambulatory BP monitoring (ABPM) or home BP monitoring (HBPM) may be used to complement standardised office BP readings for the management of high BP.
Lifestyle interventions for lowering blood pressure in patients with CKD not receiving dialysis
Sodium intake and physical activity are the two important things which have been emphasised in a lifestyle intervention.
- As per recommendation targeting a sodium intake of less than 2 g of sodium per day (or <90 mmol of Na+ per day, or less than 5 g of sodium chloride per day) in patients with high BP and CKD. Clinicians should avoid dietary sodium restriction in patients with sodium-wasting nephropathy. The risk of hyperkalemia increases in patients with advanced CKD when started on Dietary Approaches to Stop Hypertension (DASH)-type diet, or salt substitutes rich in potassium.
- As per recommendations patients with high BP and CKD to be advised to undertake moderate-intensity physical activity for a cumulative duration of at least 150 minutes per week, or to a level compatible with their cardiovascular and physical tolerance. The targets for the physical activity should be individualised as per cardio-respiratory fitness status, physical limitations and cognitive function.
Blood pressure management in patients with CKD, with or without diabetes, not receiving dialysis
- As per recommendations, adults with high BP and CKD are to be treated with a target systolic blood pressure (SBP) of <120 mm Hg, using standardised office BP measurement. The rationale behind tight control of blood pressure in CKD patients is to prevent a cardiovascular event which is a more likely outcome than end-stage kidney disease.
- Clinicians can offer less intensive BP-lowering therapy in patients with very limited life expectancy or symptomatic postural hypotension.
- As per recommendations start renin-angiotensin-system inhibitors (RASi) (angiotensin-converting enzyme inhibitor [ACEi] or angiotensin II receptor blocker [ARB]) for people with high BP, CKD, and severely increased albuminuria (G1-G4, A3) without diabetes.
- As per recommendations start RASi (ACEi or ARB) for people with high BP, CKD, and moderately increased albuminuria (G1-G4, A2) without diabetes.
- As per recommendations start RASi (ACEi or ARB) for people with high BP, CKD, and moderately-to-severely increased albuminuria (G1 to G4, A2 and A3) with diabetes.
ACEi or ARB may be considered for diabetic patients with albuminuria with normal blood pressure.
Regular monitoring of BP, serum creatinine and serum potassium within 2-4 weeks of initiation or increase in the dose of RAS blockers. Stop ACEi or ARB once the creatinine rises by more than 30% within 4 weeks following initiation or increase in dose.
Avoid these drugs in pregnant women or advise contraception in women receiving ACEi or ARB. Never combine ACEi and ARB together, or ACEi or ARB with a direct renin inhibitor.
For hyperkalemia associated with the use of ACEi or ARB, the drug should not be stopped rather measures to reduce with the use of potassium binders, moderate potassium intake or the use of diuretics should be considered.
Blood pressure management in kidney transplant recipients (CKD G1T-G5T)
As per recommendation a dihydropyridine calcium channel blocker (CCB) or an ARB to be used as the first-line antihypertensive agent in adult kidney transplant recipients. Treat adult kidney transplant recipients with high BP to a target BP of <130 mm Hg systolic and <80 mm Hg diastolic using standardised office BP measurement. Intensive blood pressure control is associated with a higher (albeit slightly) rate of loss of GFR over time in SPRINT and a higher risk of “AKI” (single, denervated kidneys may be at higher risk).
Blood pressure management in children with CKD
As per recommendation in children with CKD, 24-hour mean arterial pressure (MAP) by ABPM should be lowered to ≤50th percentile for age, sex, and height. Blood pressure to be monitored once a year with ABPM, and monitoring should be done every 3–6 months with standardised auscultatory office BP in children with CKD. In children with high BP and CKD, when ABPM is not available, manual auscultatory office BP obtained in a protocol-driven standardised setting targeting achieved SBP <90th percentile for age, sex, and height of normal children is a reasonable approach.
As per recommendation use of ACEi or ARB should be first-line therapy for high blood pressure in children with CKD. These drugs lower proteinuria and are usually well tolerated, but they carry the risk of hyperkalemia and have adverse fetal risks for pregnant women. To be avoided in children with renal artery stenosis.
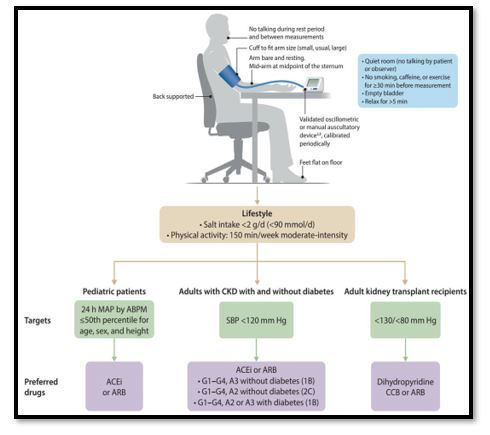
Illustration summarising the above guidelines
Disclaimer- The views and opinions expressed in this article are those of the author and do not necessarily reflect the official policy or position of M3 India.
About the author of this article: Dr Hitesh Saraogi is a diabetologist, physician and an obesity specialist at Dhanvantari Hospital, Raj Nagar Extension, Ghaziabad.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
