How to identify scorpion sting: Dr. H. Bawaskar explains
M3 India Newsdesk Sep 26, 2018
As Part 1 of the series, Dr. H. Bawaskar, well-known for his crusade against scorpion sting, rampant in rural areas throws light on identifying scorpion sting inpatients. In Part 2 read about the management of scorpion sting patients.
Abstract
Envenomation by scorpion result in a life-threatening, time-limiting cardio-respiratory emergency in human victims, yet neglected, public health disease in tropical and sub-tropical countries especially in South Africa, Middle East, Latin America and India. Irrespective of majority of different species of scorpions, they have similar cardiovascular and clinical effects.
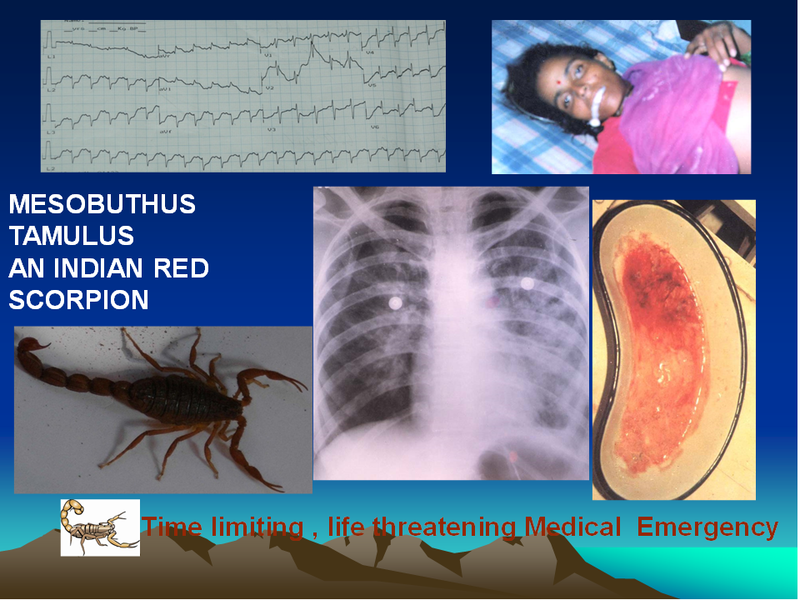
Clockwise: ECG- Sinus tachycardia and ST depression with intraventricular block; Froth in mouth due to massive pulmonary oedema; Mesobuthus tamalus (an Indian Red scorpion); Bilateral Bat wing appearance of pulmonary oedema in chest X-ray; Expectorated red oxygenated blood
Regimen including scorpion antivenom (SAV), vasodilators, has been tried. Since the advent of scorpion SAV, vasodilators, intensive care facilities and training of peripheral doctors regarding how to manage severe scorpion sting the fatality due to severe scorpion sting is significantly reduced to <1% from 30%.
Introduction
 Mesobuthus tamulus (an Indian red scorpion): Poisonous
Mesobuthus tamulus (an Indian red scorpion): Poisonous

An Indian black scorpion: Poisonous
 Palmaneus gravimanus (Big Black scorpion): Less venomous
Palmaneus gravimanus (Big Black scorpion): Less venomous
Scorpion envenomation is an occupational hazard for farmers, farm labourers, villagers, migrating population like shepherds and hunters. Envenomation by scorpions results in a life-threatening, time limiting, cardio-respiratory emergency in human victims. Irrespective of a majority of different species of scorpions, envenomation has similar cardiovascular and clinical effects.
Nearly 1000 species of scorpions are known worldwide, which belongs to six families. However, only the scorpion belonging to the family Buthidae, secretes a neurotoxic venom that is toxic to humans. Around 89 species of this family are found in India. Mesobuthus (M) tamulus, an Indian red scorpion is the most lethal species present all over India.
Envenomation by M.Tamulus is fatal if not treated properly in time. Length of this species is 2.5 to 4 inches. Its claws are red coloured, tail, legs and body is khaki-coloured. Tail consists of stout segments of these last segment end in a bulb contains two telsen modified salivary glands which secrete venom at the time of sting injected by a stinger. The stinger is short and sharp 3 to 4 mm long, enabling it to deposit the venom skin deep (the full thickness of human skin is 1.5 mm).
Skin circulation is sluggish and normally remain quiescent. Scorpion venom delays the closing of neuronal sodium channels result sudden pouring endogenous catecholamines result in “Autonomic” alpha receptors stimulations plays an important role in the pathogenesis of cardiovascular manifestations. Venomous scorpions can be identified by the thickness of pincers and tail. If pincer of claws is slender and tail consists of thick and stout segments, the scorpion is venomous. An Indian red and black scorpion can be seen in the coastal regions and rest of Maharashtra.
Scorpion venom and pathophysiology
Scorpion venom is a cocktail of several toxins. Multiple toxins may be present in the venom of a single species of scorpion capable to produce a potent synergic effect in victim. Neurotoxins of scorpion venom content highly lethal than snake venom.
The LD50 of some scorpion neurotoxins have been analyzed to be ten fold more potent than cyanide. Iberiotoxin and tamulotoxin content of scorpion Mesobuthus tamulus venom are the only selective inhibitors of potassium channel and blocking effects of scorpion toxins on potassium channels the action potential across excitable cell membrane becomes prolonged.
Sodium and potassium channel toxins of scorpion venom mediate synergistic effects responsible for intense and persistent depolarization of autonomic nerves with massive release of autonomic neuromuscular neurotransmitter evokes an ”autonomic storm”. The stimulation of nitrergic nerves supplying penile smooth muscle may explain the priapism observed in severe scorpion envenomation.
In an experimental study, sustained catecholamine decrease was recorded despite re-envenomation. Prolonged or repeated sympathetic stimulation is blunted because of exhaustion of catecholamines store. Injection of Mesobuthus tumulus venom in rat elicited initial transient hypotensive effects (cholinergic) and secondary prolonged hypertensive effects (adrenergic) effects. The hypertensive effects are venom dose-dependent.
Scorpion toxins have proved to be extremely versatile tools in ion channel research. In severe scorpion sting victims continuous, prolonged stimulation of sodium neuronal channels by Mesobuthus tamulus venom results in paralysis and cardiac neuronal sodium channel manifests Brugada syndrome. Perhaps, a drug derived from scorpion toxin could increase the sodium current, and treat the Brugada syndrome.
Asian black scorpion belonging to Scorpionidae family flourish in South-East-Asia. High concentration of nor-adrenaline and acetylcholine contents of scorpion venom account for localizing the algesic effect of acetylcholine. Role of nor-adrenaline could also explain the prolonged local burning pain, oedema, sweating, and fasciculation at the site of the sting.
Clinical manifestations
 Severe priapism due to scorpion sting. Clockwise: profuse sweating; Blood-stained expectoration in acute pulmonary oedema; Ropy salivation; Cold extremities
Severe priapism due to scorpion sting. Clockwise: profuse sweating; Blood-stained expectoration in acute pulmonary oedema; Ropy salivation; Cold extremities
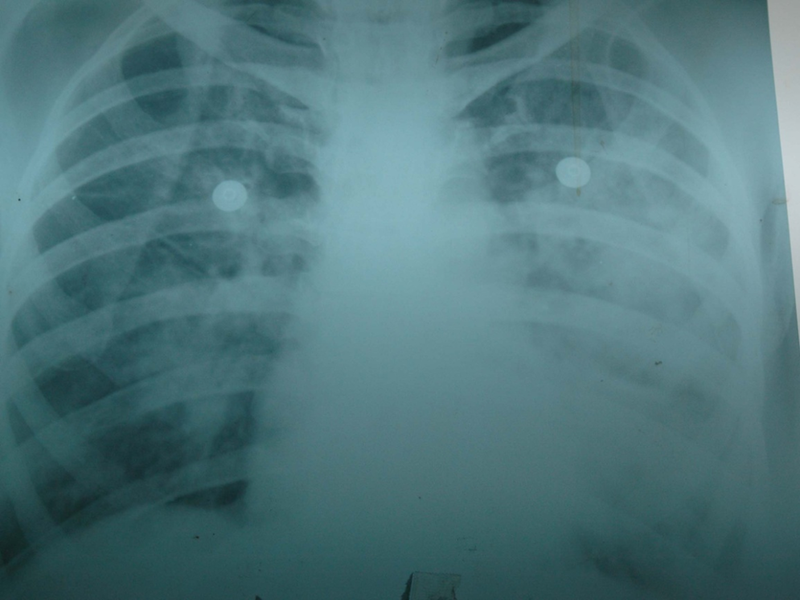 Bilateral pulmonary oedema
Bilateral pulmonary oedema
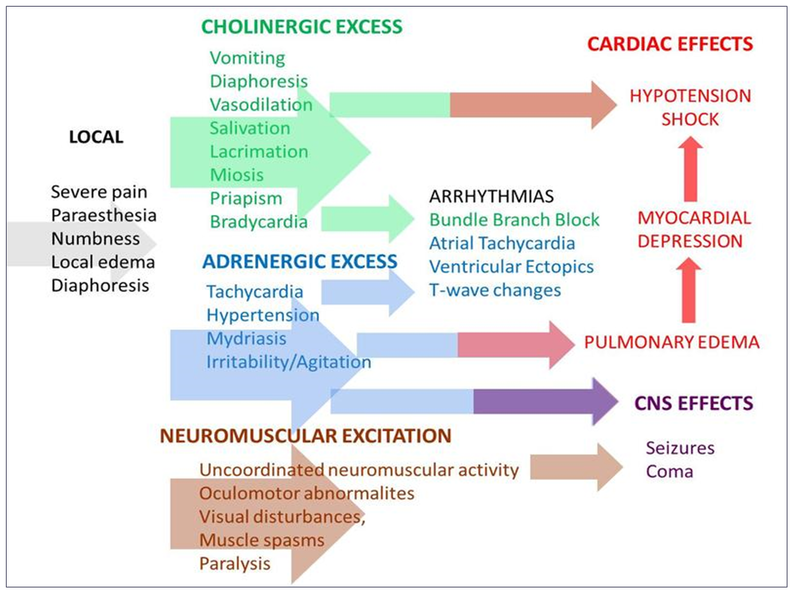
Pathophysiology of scorpion evenomation
Severity of envenoming depends upon the species of scorpion, lethality and dose of venom injected at the time of sting. Severe effects are seen in the first victim than envenomed by the same scorpion immediately to a subsequent victim. This confirms that severe local pain without sign and symptoms of autonomic storm suggestive of minimum envenoming. Severity of envenoming is related to age of victim, size, species of scorpion and season of the sting and time elapsed between sting and hospitalisation.
Children are more prone for severe manifestation with 3 to 5% fatality irrespective of intensive care management. Clinically “autonomic storm” evoked due to envenoming by venomous scorpion species is characterized by transient parasympathetic (vomiting, profuse sweating, ropy salivation, lacrimation, bradycardia, ventricular premature contraction, priapism in male, hypotension) and prolonged sympathetic (cold extremities, hypertension, tachycardia, pulmonary oedema and shock) stimulation. Both twigs of autonomic nervous system are stimulated simultaneously, thus clinical presentation varies.
On basis of clinical manifestations at the time of arrival to hospital and according to severity they are graded in four grades.
- Grade 1- Severe excruciating local pain at the sting site radiating along with corresponding dermatomes, mild local oedema with seating at the sting site, without systemic involvement.
- Grade 2- Signs and symptoms of autonomic storm characterised by acetyl choline excess or parasympathetic and sympathetic stimulation.
- Grade 3- Cold extremities, tachycardia, hypotension or hypertension with pulmonary oedema, respiratory rate >24 per minute, and basal rales or crackles in lungs.
-
Grade 4- Tachycardia, hypotension with or without pulmonary oedema with warm extremities (warm shock).
A-Local manifestations
- Soon after the sting, the patient experience severe excruciating radiating pain from sting site usually toes and fingers. Inconsolable, incessant crying in a child which is a sudden onset is a diagnostic sign of scorpion sting.
- Due to pain there is transient bradycardia, rise in blood pressure, mild sweating but extremities are warm.
- Sudden tap at and around the site of sting induces severe pain and withdrawal is a diagnostic sign of sting called “TAP sign”.
- Severe pain without systemic involvement is suggestive of a benign or dry sting by venomous species.
- Oedema and inflammation at the sting site blunt the sodium channel blocker action of lidocaine. Infiltration of single dose 1.5 to 2 ml of lidocaine without adrenaline around the sting site, oral acetaminophen or NSAID, cold therapy at the sting site and oral diazepam make the victim more comfortable.
- Pain conduction is blunted and it is tolerable or mild due to vasoconstriction caused by liberated circulating catecholamine due envenoming by venomous species.
- Reappearance of severe pain accompanied by improved peripheral circulation by vasodilatation is suggestive of recovery.
- Local incision, tight tourniquet, application of potassium permanganate, herbal remedies lead to herbal toxicity, local tissue damage, infection and gangrene.
Systemic manifestations
- Vomiting: Transient projectile vomiting is due to autonomic storm often seen in a patient envenomed by Mesobuthus tamulus. Vomiting is due to serotonin content of venom and acetylcholine excess.
- Profuse sweating: Sweat literally flows all over the body. Clinically it is called “skin diarrhoea”. Sweating persists for 3 to 17 hours (this was observed before availability of scorpion antivenom).
- Salivation: Thick ropy salivation due to stimulation of bronchial mucous glands, difficult to expectorate occurs soon after sting and it persists for 2 to 4 hours. Excessive salivation and bronchial secretion are indirect contributing factors for respiratory failure, clinical presentations like organophosphate poisoning.
- Priapism: It is seen in almost all victims of pediatric age group and 20% adults. Priapism is diagnostic of venomous envenoming but its absence or disappearance does not correlate with the outcome. It persists for 5 to 16 hours.
Thus, vomiting, profuse sweating, salivation, and cool skin priapism are cardiac premonitory diagnostic signs and symptoms of scorpion sting suggestive of free circulating venom in the blood accessible to antivenin therapy.
- Cold extremities: They are due to severe vasoconstriction due to liberated circuiting catecholamine. Cold extremities persist for 12 to 26 hours. The skin over the palm and dorsum because of water- logging will look like a washerman’s hand. Cold extremities are accompanied by severe cardiovascular manifestations. Recovery is indicated by improvement in skin temperature and recurrence of severe local pain at the sting site which was mild on arrival.
- Mydriasis- Poorly dilated or non-reacting pupils are often seen in the early phase of an autonomic storm and associated with raised blood pressure. Papillary effects are due to alpha receptor stimulation of dilator papillary muscles by excessive circulating catecholamine or preganglionic release of acetylcholine and post-ganglionic sympathetic stimulation.
Cardiovascular system (CVS) manifestations
CVS is mostly affected by venomous sting. Clinical manifestations depend upon the duration of envenoming. Hypertension, cardiac arrhythmias, tachy-bradycardia, pulmonary oedema, hypotension, and shock are not different syndromes but one process of an ongoing autonomic storm.
Hypertension
- Around 45 to 70% of victims within 30 minutes to 8 hours of a sting will report raised blood pressure ranging from 140/90 to 200-230/130-160 mmHg and Bradycardia (heart rate of 42-58 per minute).
- Main complaints would be of a headache, chest discomfort, suffocation, per oral and extensive paresthesia due to ongoing vasoconstriction.
- Clinical examination will show para-sternal systolic lift, apical bulge, proto-diastolic gallop, and transient-grade 2/6 apical systolic murmur of mitral regurgitation due to papillary muscle dysfunction.
- Children will look agitated, confused, and have propped-up eyes, oculogyric phenomenon, puffy face, decreased level of consciousness, and convulsions; manifestations of encephalopathy with blood pressure measurements between 95 and 99 percentiles for age and sex of the child.
- If untreated, the hypertensive effect will be long-lasting, and it would result in the development of myocardial failure and pulmonary oedema.
- Hyper-renin and sympathetic stimulation results in a rapid and significant increase level of epinephrine, nor-epinephrine, endothelin, atrial natriuretic peptide due to sting by the Buthidae species.
- Accumulation of angiotensin II accelerates myocardial injury and oxygen demand. Alpha receptors stimulation plays an important part in the pathogenesis of hypertension and pulmonary oedema due to the scorpion sting.
Tachycardia
- Around 15-20% cases reported after 6-7 hours of sting develop supraventricular tachycardia (heart rate 110-240 per minute). At times, sudden onset of tachycardia occurs in a recovering hospitalised patient due to relapse as a result increased circulation due to treatment with vasodilators or severe ongoing myocardial injury and beta receptors stimulation due to the re-absorption of venom from the sting site which act as a depot.
- However, marked tachycardia occurs after 10-12 hours of hospitalisation with hypotension accompanied with warm extremities with or without pulmonary oedema, suggestive of warm shock with gray or cadaveric pallor. Impaired left ventricular filling, reduction in cardiac output due to marked tachycardia particularly in children results in delirium and convulsions due to anoxia to the brain.
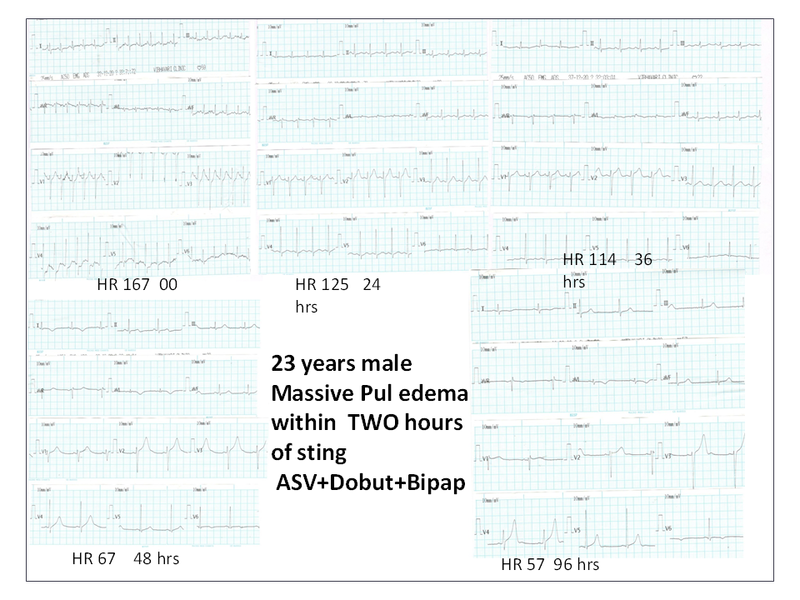 Marked tachycardia with subsequent reduction in heart rate and improvement
Marked tachycardia with subsequent reduction in heart rate and improvement
Hypotension
- Initial hypotension is for short periods initially due to hypovolemia because of vomiting, sweating, salivation, and cardiac arrhythmias. Delayed long lasting hypotension can be attributed to the reduction in systemic vascular resistance, a hypokinetic phase accompanied by a raised heart rate, hypotension with shock reflecting an altered left ventricular contractility. The venom stimulates kinase II enzyme that can lead to the accumulation of bradykinin a neuromuscular agent incriminated for development of pulmonary edema and hypotension.
- In a hospitalised patient, on the 2nd or 3rd day of admission, asymptomatic hypotension with bradycardia but good volume pulse with warm extremities accompanied with pronged QTc interval attributed to the depletion of catecholamines from nerve terminals because of autonomic storm can be observed. It is a self-limiting phenomenon and does not need any intervention, because irrespective of hypotension and bradycardia, the patient will be asymptomatic and recovery natural accompanied with clinical improvement.
Pulmonary oedema
- Around 19-20% victims develop pulmonary edema within 30 minutes with severe hypertension and may develop after 36 hours of the sting, along with hypotension and tachycardia.
- It is clinically characterised by the acute onset of dyspnea (respiratory rate >24 per minute), air hunger in children, prominent inter-costal withdrawing, tachycardia, summation gallop, systolic murmur, cold extremities, sudden onset of an intractable cough, bilateral moist rales and low-volume fast thread pulse.
- During the month September and October cases may manifest sudden onset of massive pulmonary oedema with central cyanosis, intractable cough with continuous expectoration of blood stain froth from mouth and nostril. Reduction in SPO2 concentration. The earliest sign of developing pulmonary oedema is cough.
Neurological manifestations
Mesobuthus tamulus envenoming may cause focal and neurological presentation including hemi paresis, hemorrhagic or thrombotic stroke.
Acute Pancreatitis
Pancreatitis due to scorpion sting is rare in India. One should suspect in case of persistent tachycardia, shock , abdominal colic accompanied with raised level of amylase. In autopsy finding extensive necrosis and haemorrhage suggestive of haemorrhagic pancreatitis.
Fatality
Death within 30 minutes of a sting can occur due to lethal ventricular arrhythmia. High fatality due to scorpion sting in India is attributed to delay in reporting to the hospital due to poor transport. At times, the medical officer is not aware of a western line of treatment or he may have never treated severe scorpion sting before.
- Atropine increases the severity of pulmonary oedema.
- Steroids increase the necrotizing effects of circulating catecholamines and oxygen demand of myocardium.
- Digitalis enhances already increased myocardial contraction and oxygen requirement. Antihistamines and venom, both acts synergistically by inhibiting Ca+ dependent potassium activating channels leading to QTc prolongation and may cause sudden death
Moreover, the actual transport of severe scorpion sting cases to nearest big hospital delays the treatment and adds to the number of deaths.
Part 2 of the series- How to manage scorpion sting patients- Dr. H Bawaskar explains
The writer, Dr. Himmatrao Bawaskar is a renowned Indian physician with publications in The Lancet. He has done extensive research in scorpion sting- diagnosis and treatment protocol.
Disclaimer- The views and opinions expressed in this article are those of the author's and do not necessarily reflect the official policy or position of M3 India.
The author did not accept any payment for the article.
-
Exclusive Write-ups & Webinars by KOLs
-
 Daily Quiz by specialty
Daily Quiz by specialty -
 Paid Market Research Surveys
Paid Market Research Surveys -
Case discussions, News & Journals' summaries
